A high yield is only one part of the story when it comes to picking dividend stocks.
It is tempting for a dividend investor to simply select the highest yielding stocks. The problem with that approach is that it exposes you to the risk of dividend cuts if the yield is too high for the company to support.
Which is why dividend lovers also need to consider dividend history as they look at a company. And, when you do that, you’ll find that companies like Pfizer(PFE -0.50%), which has a huge 7.2% yield, don’t match up to companies like Johnson & Johnson(JNJ 1.03%), Omega Healthcare(OHI -0.50%), and Merck(MRK -0.03%).
Here’s what you need to know about these three healthcare dividend stocks.
Image source: Getty Images.
1. If you need the money to live, dividend reliability is key
Pfizer is actually a well-run company. Sure, it is facing hard times right now, but it has dealt with difficult periods before and survived. It is highly likely that it will do so again, noting that some of the issues it is dealing with are a natural part of the pharmaceutical industry. For example, patent expirations are on the horizon, and it needs to find new drugs to replace older ones. Investors rightly worry about such patent cliffs, but they aren’t the least bit unusual for drug makers.
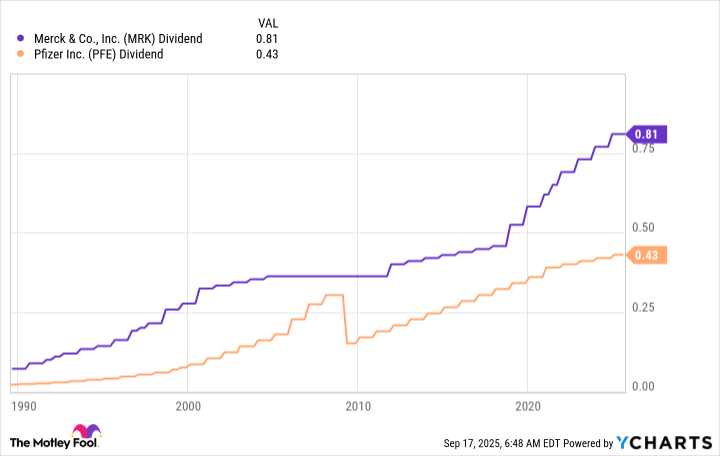
That said, Pfizer’s huge 7.2% dividend yield is also a reflection of the downbeat view among regulators and consumers around vaccines. So there’s more to watch here than the normal industry swings. But the same things could, largely, be said of Merck, one of Pfizer’s competitors. The drugs and vaccines in question are different, but the worries are basically the same. You could easily buy either one if you wanted exposure to the pharma sector. Why pick Merck and its less impressive, though still high, 4% yield?
The answer is simple. Merck has a long history of supporting its dividend even through difficult periods. Pfizer cut its dividend in 2009 when it bought Wyeth. The acquisition was good for Pfizer, but the dividend cut was terrible for income investors. If dividend consistency matters to you, Merck wins here.
2. Omega Healthcare has survived the hardest of times
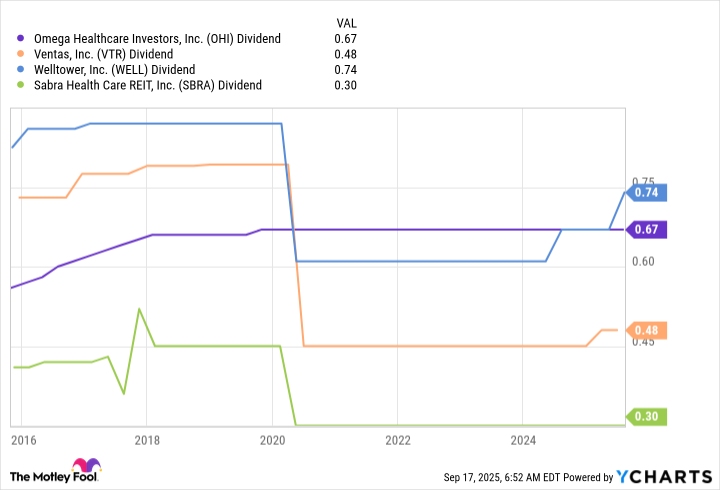
If Merck’s dividend resilience over time impresses you, you’ll probably find Omega Healthcare even more exciting. The company owns senior housing facilities, which were hard hit during the COVID-19 pandemic. To put it simply, older people in group settings were at severe risk of dying from the pandemic. That had the exact negative impact you would expect on nursing homes and similar properties. And yet Omega Healthcare, a senior housing-focused real estate investment trust (REIT), didn’t cut its dividend like many of its competitors.
It didn’t raise the dividend, either, but it did stand behind the payment, realizing that investors were relying on that quarterly check. That should make Omega’s nearly 6.4% yield look a lot more attractive, even for more conservative dividend investors.
And don’t forget that the pandemic is now mostly in the rearview mirror. The second quarter of 2025 saw Omega invest in new assets, which should help spur growth and post an 8% year-over-year increase in adjusted funds from operations (FFO). With the business looking like it is on the mend, the dividend is likely more secure now than it has been in years.
3. The Dividend King approach
If you are looking to stick to only the most reliable of dividend companies, however, then you’ll want to buy a Dividend King. These are stocks that have raised their dividends for over 50 years. Johnson & Johnson’s string of over 60 annual dividend increases makes it the healthcare stock to beat when it comes to dividend reliability. Of course, investors know how reliable this drug and medical device maker is, so the stock is usually afforded a premium valuation. Right now, the yield is around 3% or so, the lowest on this list. However, it is still higher than the 1.7% yield of the average healthcare stock, making J&J a good pick for investors who place a high value on dividend consistency.
Clearly, Johnson & Johnson has its own warts to consider. For example, it faces all of the same issues in the pharma space as Merck and Pfizer. It is also dealing with a lingering class action lawsuit around talcum powder that it once sold. So even this Dividend King isn’t risk-free. But if history is any guide, you can count on the dividend continuing to be paid through thick and thin.
Don’t just jump at the highest yield
Although there’s nothing particularly wrong with Pfizer, a comparison to Merck, Omega, and J&J shows that a high yield isn’t the only factor you should consider if you are looking for a good dividend stock. If reliable dividend stocks are what you want populating your dividend portfolio, you will clearly want to look past Pfizer’s yield. And when you do that, you’ll likely find that Merck, Omega, and Johnson & Johnson all offer a more compelling combination of income reliability and yield.
Why is the healthcare industry a great place to find investments right now?
There are tree major reasons. First, spending on healthcare in the U.S. is growing rapidly. The industry already accounts for more than 17% of the economy and is expected to expand by 5.8% a year on average through 2033, when it should account for more than a fifth of the economy.
Second, the healthcare industry is widely considered to be recession-proof, or at least highly recession-resistant. Historically, the sector has fared well during recessions, as people need healthcare and find ways to pay for it even when the economy is contracting.
And the third reason is demographics. U.S. society is graying. The number of Americans 65 or older is projected to rise from 62 million in 2024 to 84 million within three decades, and the number of centenarians — those 100 or older — is expected to quadruple over that time frame. It’s no secret that people generally require more healthcare as they age.
A health giant
So, what’s a good way for an investor to take advantage of these trends and participate in that industry’s relentless expansion? There are many ways, including investing in drug manufacturers, medical device makers, health insurers, and care providers, among other health-related companies.
One health company has operations that span many of those sectors. In fact, you might have visited one of its locations in the past month. It has around 9,600 stores across all 50 states plus the District of Columbia and Puerto Rico, and 85% of Americans live within 10 miles of one.
I’m talking about CVS Health(CVS 0.43%). CVS is much more than a pharmacy chain. It provides healthcare services like lab tests, health screenings, vaccinations, and treatments for minor injuries at its in-store clinics. It employs more than 40,000 physicians, pharmacists, nurses, and nurse practitioners to enable those services.
It also owns health insurer Aetna, which it acquired in 2018. Covering 36 million people, it’s the fifth-largest health insurer in the nation.
Oh, and the pharmacy part: CVS Health has a 27% share of pharmacy prescriptions nationwide.
Image source: Getty Images.
Strong results
Right now, CVS is firing on all cylinders. The company released its second-quarter results on July 31, and both earnings and revenue beat Wall Street’s estimates. The company also increased its guidance for full-year earnings per share from a range of $6.00 to $6.20 to a range of $6.30 to $6.40. The report sent the stock sharply higher, and it climbed 18% in August.
Analysts now expect full-year earnings growth of 15% in 2025 and another 13% in 2026.
Yet the stock remains cheap, trading at just 10 times forward earnings estimates, which is lower than many of its healthcare industry peers.
CVS is also expanding. It’s now swallowing up many former locations of competitor Rite Aid, which filed for bankruptcy protection in May, and even better, acquiring Rite Aid’s prescription files.
CVS has a market cap of about $90 billion, and the stock is up 65% year to date as of market close Sept. 10. Looking back further paints a different picture. The stock is down roughly 30% over the past three years. But the company has been rewarding investors. Last year, the company repurchased about 40 million shares of stock and paid $3.3 billion in dividends.
Now on sale
So, CVS is doing well, and shares are on sale. They dipped a bit recently when CVS executives declined to give guidance about upcoming government ratings that will impact how much money the company gets from Medicare Advantage plans.
But that’s not worrisome. CVS says it never gives guidance between quarterly earnings reports.
Savvy investors will take this opportunity to pick up a few shares of the expanding healthcare provider in light of the company’s potential. There’s plenty of upside with CVS.
WASHINGTON — Senate Democratic Leader Charles E. Schumer weathered backlash from Democrats earlier this year when he voted with Republicans to keep the government open. But he’s now willing to risk a shutdown at the end of the month if Republicans don’t accede to Democratic demands.
Schumer says he and House Democratic Leader Hakeem Jeffries are united in opposing any legislation that doesn’t include key healthcare provisions and a commitment not to roll them back. He argues that the country is in a different place than it was in March, when he vigorously argued against a shutdown, and he says he believes Republicans and President Trump will be held responsible if they don’t negotiate a bipartisan deal.
“Things have changed” since the March vote, Schumer said in an interview with the Associated Press on Thursday. He said Republicans have since passed Trump’s massive tax breaks and spending cuts legislation, which trimmed Medicaid and other government programs, and Democrats are now unified — unlike in March, when he voted with Republicans and Jeffries voted against the legislation to fund the government.
A shutdown, Schumer said, wouldn’t necessarily worsen an environment in which Trump is already challenging the authority of Congress. “It will get worse with or without it, because Trump is lawless,” Schumer said.
Democrats’ consequential decision
Schumer’s threat comes as Republicans are considering a short-term stopgap spending measure to avoid a Sept. 30 shutdown and as Democrats face what most see as two tough choices if the parties can’t negotiate a deal — vote with Republicans to keep the government open or let it close indefinitely with no clear exit plan.
It also comes amid worsening partisan tensions in the Senate, where negotiations between the two parties over the confirmation process broke down for a second time on Thursday and Republicans are changing Senate rules to get around Democratic objections to almost all of Trump’s nominees. Democrats are also fuming over the Trump administration’s decision to unilaterally claw back $4.9 billion in congressionally approved foreign aid just as negotiations over the spending deadline were getting underway in late August.
Republicans move ahead
Republicans say that Democrats clearly will be to blame if they don’t vote to keep the government open.
Trump said Friday to not “even bother” negotiating with Democrats. He said Republicans will likely put together a continuing resolution to keep funding the federal government.
“If you gave them every dream, they would not vote for it,” Trump said, adding “we will get it through because the Republicans are sticking together.”
Senate Majority Leader John Thune (R-S.D.), said in an interview with Punchbowl News on Thursday that he believes Democrats see it as “politically advantageous” to have a shutdown.
“But they don’t have a good reason to do it,” Thune said in the interview. “And I don’t intend to give them a good reason to do it.”
Thune has repeatedly said that Schumer needs to approach Republicans with a specific proposal on healthcare, including an extension of expanded government tax credits for many Americans who get their health insurance through the Affordable Care Act. Some Republicans are open to extending those credits before they expire at the end of the year, but Thune has indicated that he is unlikely to add an extension to a short-term spending bill, instead favoring a “clean” stopgap for several weeks without any divisive issues while Congress finishes its budget legislation.
Schumer said he believes his caucus is ready to oppose the stopgap measure if Republicans don’t negotiate it with Democrats. “I think the overwhelming majority of our caucus, with a few exceptions, and same with the House, would vote against that,” he said.
Less realistic is Democrats’ demand that Republicans roll back Medicaid cuts enacted in their tax breaks and spending cuts legislation this summer, what Trump called his “big, beautiful bill.”
Escalating partisan tensions over spending
Schumer said Democrats also want Republicans to commit that the White House won’t take back money they have negotiated and Congress has approved after Republicans pushed through a $9-billion cut requested by the White House in July and Trump blocked the additional foreign aid money in August. “How do you pass an appropriations bill and let them undo it down the road?” Schumer said.
Congress is facing the funding deadline Sept. 30 because Republicans and Democrats are still working out their differences on several annual budget bills. Intractable partisan differences on an increasing number of issues have stalled those individual bills in recent years, forcing lawmakers to pass one large omnibus package at the end of the year or simply vote to continue current spending.
A shutdown means federal agencies will stop all actions deemed nonessential, and millions of federal employees, including members of the military, won’t receive paychecks. The most recent shutdown — and the longest ever — was during Trump’s first term in 2018 and into 2019, when he demanded money for his U.S.-Mexico border wall. It lasted 35 days.
Schumer’s March vote
Schumer’s move to support the spending legislation in March put him in the rare position of bucking his party’s base. He said then that of two bad options, a partial government shutdown was worse because it would give Trump even more control to lay off workers and there would be “no offramp” to get out of it. “I think people realize it’s a tough choice,” he said.
He faced massive backlash from within the party after the vote, with some activists calling on him to resign. Jeffries temporarily distanced himself from his New York colleague, saying in a statement immediately after Schumer’s vote that House Democrats “will not be complicit.” The majority of Senate Democrats also voted against the GOP spending legislation.
This time, though, Schumer is in lockstep with Jeffries and in messaging within his caucus. In Democrats’ closed-door lunch Wednesday, he shared polling that he said suggested most Americans would blame Trump, not Democrats, for a shutdown.
“I did what I thought was right” in March, Schumer said. “It’s a different situation now than then.”
Jalonick writes for the Associated Press. AP writer Christopher Megerian contributed to this report.
Experts who follow these stocks think they can fly higher despite already gaining over 100% since the end of July.
Investors in search of stocks that can produce dramatic gains in a short time frame will want to turn their heads toward the healthcare sector. A handful of stocks in the space more than doubled in price recently.
Shares of Precigen(PGEN -4.61%) and Mineralys Therapeutics(MLYS 4.86%) have already risen more than 100% since the end of July. Despite the recent run-ups, Wall Street experts who follow these stocks believe they could soar even further.
Image source: Getty Images.
1. Precigen
From the end of July through Friday, Sept. 5, shares of Precigen shot 155% higher. The market cheered because the drugmaker earned approval from the Food and Drug Administration (FDA) for its first treatment. Papzimeos is a cell-based immunotherapy for the treatment of recurrent respiratory papillomatosis (RRP), a rare disease that results in tumors lining the respiratory tract.
Papzimeos is the first and only treatment approved by the FDA to treat an estimated 27,000 patients with RRP. The agency granted the drug full approval instead of waiting for a confirmatory study. In the single-arm trial supporting its application, 18 out of 35 patients responded well enough to avoid tumor removal surgery for at least 12 months after treatment with Papzimeos.
The agency and analysts following Precigen were encouraged by the fact that 15 out of the initial 18 responders remained surgery-free 24 months after treatment with Papzimeos. In response, Swayampakula Ramakanth from HC Wainwright reiterated a buy rating and an $8.50 price target that implies a 95% gain in the year ahead.
2. Mineralys Therapeutics
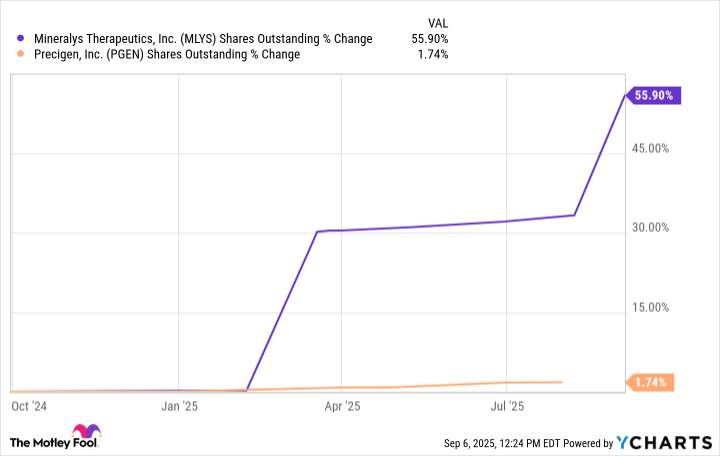
Shares of Mineralys Therapeutics rose 146% from the end of July through Sept. 5. Investors were excited about a successful new funding round to support continued development of lorundrostat, its lead candidate. On Sept. 2, Mineralys suspended an at-the-money equity offering and, within a couple of days, completed a secondary offering that ended up raising $287.5 million.
In August, investors hardly noticed a presentation of phase 3 trial results regarding lorundrostat. Patients who added the aldosterone inhibitor to the medications they were already taking reduced their systolic pressure by 16.9 millimeters of mercury after six weeks on treatment, compared to just 7.9 millimeters of mercury for patients who received a placebo.
Mineralys’ stock shot higher after AstraZeneca reported arguably inferior 12-week data for an aldosterone inhibitor it’s developing called baxdrostat. At week 12, it reduced patients’ systolic pressure by 15.7 millimeters of mercury, compared to 5.8 millimeters of mercury for the placebo group.
Less than a week ahead of Mineralys’ successful secondary stock offering, Bank of America analyst Greg Harrison boosted his target for the stock to $43 per share. The raised target implies a gain of about 24% from recent prices.
Time to buy?
Before you get too excited about Mineralys and its hypertension candidate, it’s important to realize the pre-commercial-stage business finished June with $325 million in cash, or enough to last into 2027. Diluting shareholder value to raise additional capital that could now push the stock price higher means the company isn’t super confident that it can quickly submit an application and earn approval for its lead candidate before the beginning of 2027.
At recent prices, Mineralys sports a huge $2.7 billion market cap that could shrink significantly if it looks like timing will become an issue that allows AstraZeneca’s candidate to gain and maintain a large share of the market for new hypertension drugs. It’s probably best to wait and see whether this company can earn approval for lorundrostat in a timely manner before adding the stock to your portfolio.
With a market cap of $1.3 billion at recent prices, expectations for Precigen are lower than they probably should be. Papzimeos is already approved and will launch unchallenged in its niche market.
Papzimeos’ addressable patient population is small, but a list price north of $200,000 per year per patient means it could rack up more than $1 billion in annual sales at its peak. Since drugmaker stocks generally trade at mid- to high-single-digit multiples of total sales, adding some shares to a diversified portfolio now looks like a smart move.
Bank of America is an advertising partner of Motley Fool Money. Cory Renauer has no position in any of the stocks mentioned. The Motley Fool recommends AstraZeneca Plc and Mineralys Therapeutics. The Motley Fool has a disclosure policy.
The country tops the list for travellers looking for top-quality healthcare abroad, with an overall healthcare score of 78.72. The UK didn’t make the top 10 and ranked 27th out of 110.
One country scored an impressive 78.72 for their healthcare(Image: Twenty47studio via Getty Images)
Almost half of Brits are planning a winter getaway, with one in six jetting off to Asia, the Middle East, Central and South America, according to Scott Dunn Travel. However, health concerns while abroad are a worry for some holidaymakers.
New research from 1st Move International Removals has delved into healthcare options overseas. The study evaluated factors such as medicine availability and cost, government readiness, and medical infrastructure and professionals.
Shockingly, the UK didn’t even make it into the top 10, coming in at 27th out of 110 countries. The UK scored 47.15 out of 100 on the Healthcare Index, but did best in the Medical Infrastructure and Professionals category with 78.03, reports the Express.
Taiwan beat the likes of Australia and Canada to the top spot(Image: Twenty47studio via Getty Images)
So, which country offers the best healthcare for travellers?
Taiwan takes the top spot for those seeking high-quality healthcare abroad, boasting an overall score of 78.72.
With an impressive infrastructure rating of 87.16, Taiwan’s efficient medical system ensures easy access to top professionals and facilities. Its highly praised National Health Insurance (NHI) system caters to both nationals and expats, making Taiwan an ideal destination for health-conscious travellers.
South Korea takes the second spot, providing peace of mind for tourists with a robust healthcare score of 77.7. Renowned for its state-of-the-art hospitals and skilled staff, South Korea’s infrastructure scores 79.05, ensuring dependable care for visitors.
The nation’s healthcare system, which operates on a national health insurance model, also benefits expats who are eligible to enrol after six months.
Australia ranks third, offering reliable healthcare to tourists with an overall score of 74.11. With an infrastructure rating of 90.75, the country boasts some of the world’s top hospitals and professionals.
Australia offers comprehensive medical coverage for its residents through Medicare, including GP appointments and hospital visits. For expats, a two percent Medicare Levy is applicable.
The UK came a disappointing 27th (Image: Getty)
Here are the top 10 countries offering the best healthcare for travellers:
Former Vice President Kamala Harris’ decision to forgo a run for California governor has created a wide-open race in next year’s election to run the nation’s most populous state, according to a poll released Tuesday by UC Berkeley and the Los Angeles Times.
Nearly 4 in 10 registered voters surveyed said they are uncertain about whom they will support in the 2026 contest to replace termed-out Gov. Gavin Newsom.
“It’s very unsettled. Most of the voters, the plurality in this poll, are undecided,” said Mark DiCamillo, director of the poll, which was conducted by UC Berkeley’s Institute of Governmental Studies and co-sponsored by The Times. “They don’t really know much about the candidates.”
Share via
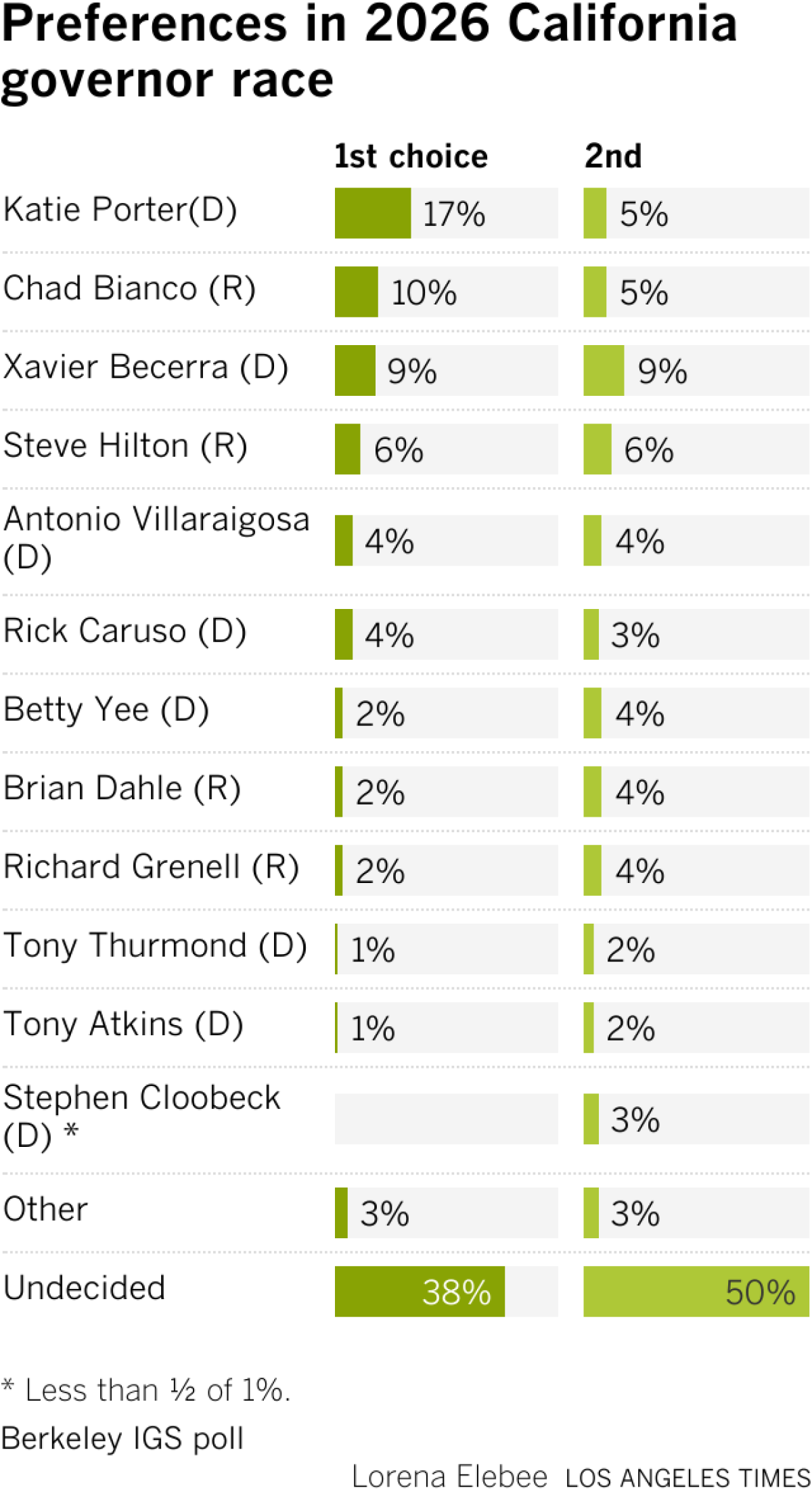
Among those who had a preference, former Democratic Rep. Katie Porter of Irvine had a small edge as the top choice, with the backing of 17%. Riverside County Sheriff Chad Bianco, a Republican, was the only other candidate who received double-digit support, winning the backing of 10% of respondents.
DiCamillo said Porter’s unsuccessful 2024 U.S. Senate campaign boosted her recognition among California voters, but cautioned that she had a small, early lead more than nine months before the June 2 primary. Bianco’s support was driven by voters focused on crime and public safety, taxes and the budget deficit, perennial concerns among GOP voters, according to the survey.
Other top candidates for governor — former U.S. Health and Human Services Secretary Xavier Becerra, former Los Angeles Mayor Antonio Villaraigosa, former state legislative leader Toni Atkins, current California Supt. of Public Instruction Tony Thurmond, former state Controller Betty Yee, wealthy businessman Stephen Cloobeck and conservative commentator Steve Hilton — received single-digit support as voters’ first choice in the poll. A few potential candidates also had single-digit support, including billionaire Los Angeles businessman Rick Caruso, former Trump administration official Ric Grenell and former GOP state Sen. Brian Dahle.
The survey is among the first independent public polls since Harris announced in late July that she would not run for governor in 2026, dramatically reshuffling the calculus in a crowded race that the former vice president was widely expected to dominate if she mounted a campaign. The poll also took place after Lt. Gov Eleni Kounalakis dropped out of the contest this month to run for state treasurer instead.
“It’s pretty wide-open,” DiCamillo said. “And when you look at the second-choice preference, first and second together, it’s bunched together.”
When voters were asked to rank their top two choices, Porter received 22% as the first or second choice, Becerra got 18%, Bianco notched 15% and Hilton won 12%, according to the poll.
None of the politicians running are well known by Californians compared with the state’s last three governors: Newsom, the former mayor of San Francisco and lieutenant governor, who during his two terms as governor has positioned himself as a foil to President Trump ; former two-term Gov. Jerry Brown, who along with his father left an indelible imprimatur on California’s history; and former Gov. Arnold Schwarzenegger, a global celebrity who returned to the Hollywood limelight after he left office, along with launching efforts to fight climate change and support independent redistricting nationwide.
A pressing question is whether anyone else enters the race, notably Caruso, who has the ability to self-fund a campaign. The deadline to file to run for the seat is March 6.
Whoever is elected as California’s next governor will face the difficult task of contending with a hostile Trump administration and an electorate looking to the state’s next leader to address its most pressing concerns.
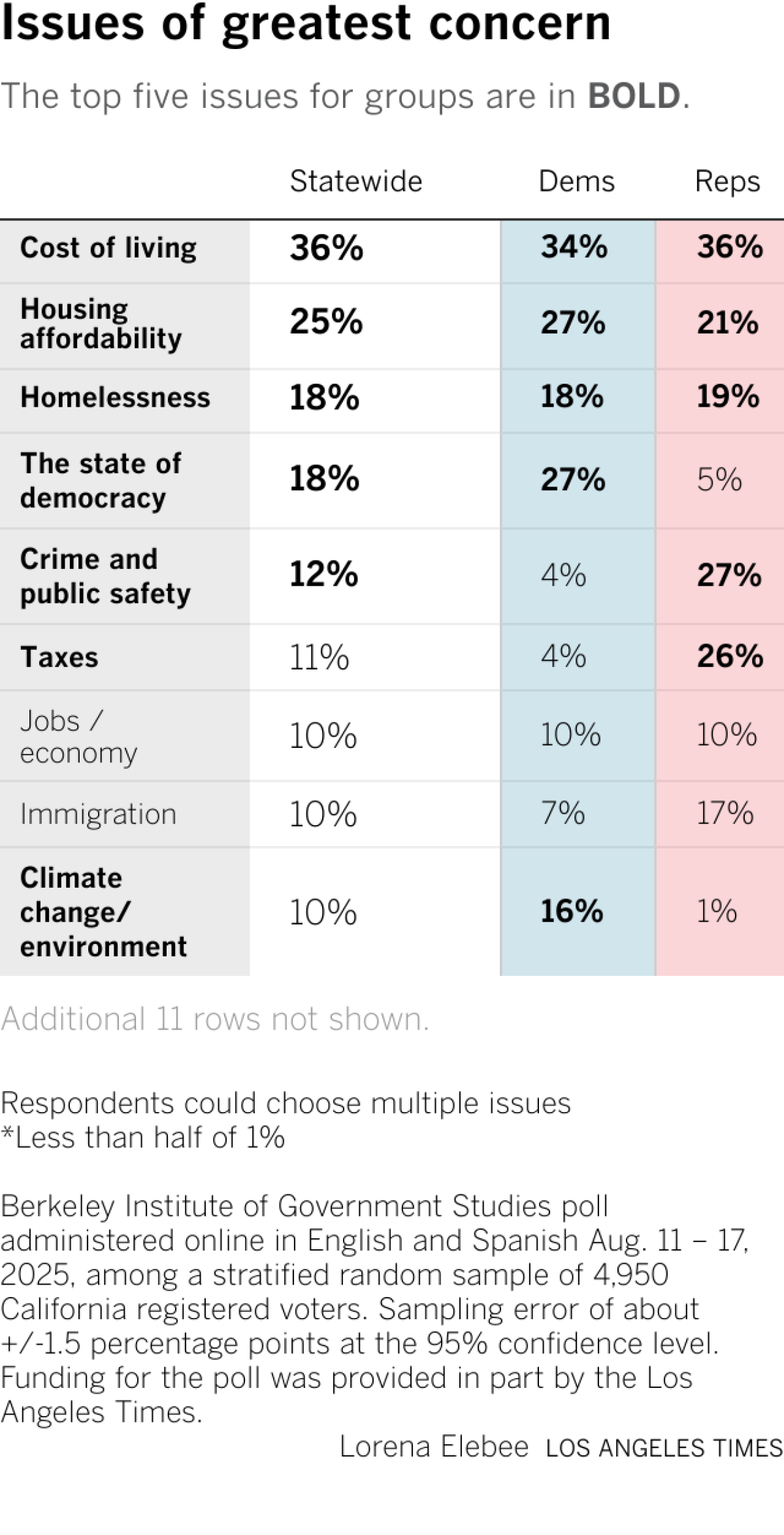
Economic issues are top of mind among all registered voters, with 36% saying the cost of living is their greatest concern and 25% focusing on the affordability of housing, according to the poll. But there were sharp partisan disparities about other issues. Democrats were more concerned about the state of democracy, climate change and healthcare, while Republicans prioritized crime, taxes and immigration.
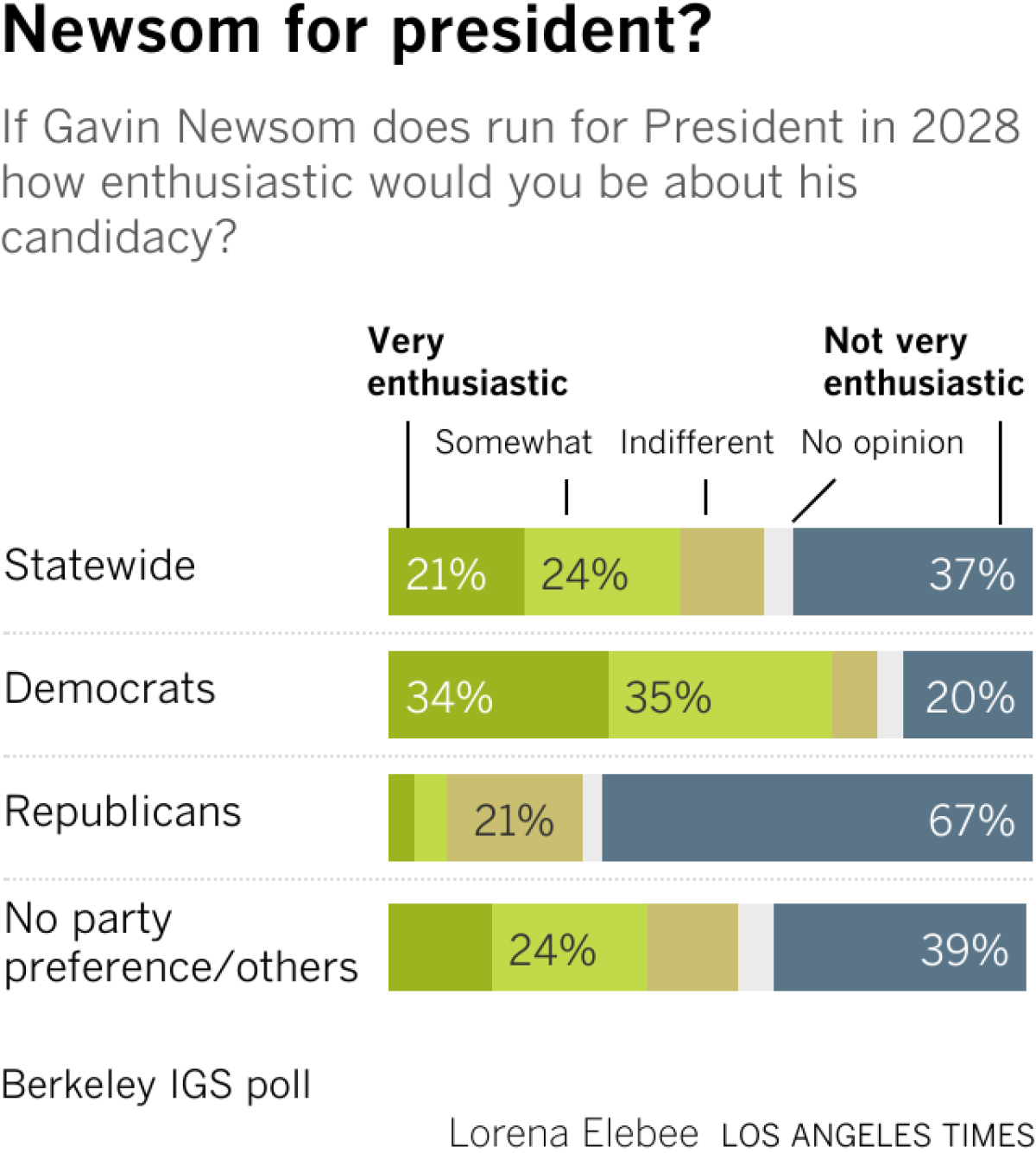
Two of California’s most prominent Democrats, Newsom and Harris, are longtime friends grounded in their Bay Area roots and both viewed as potential 2028 presidential candidates.
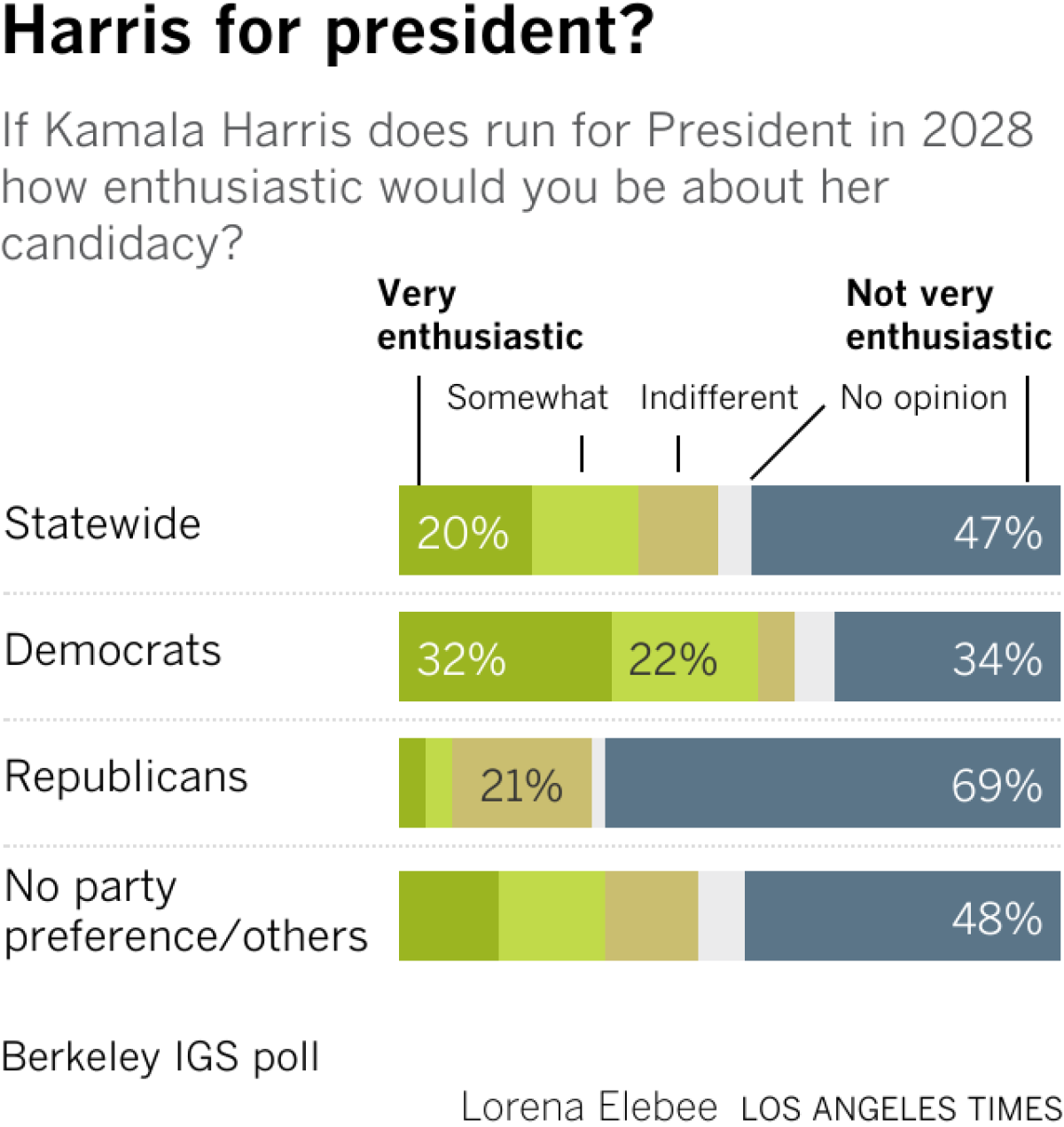
As a potential White House hopeful, Newsom has an edge over Harris among Californians overall as well as the state’s Democrats, according to the poll.
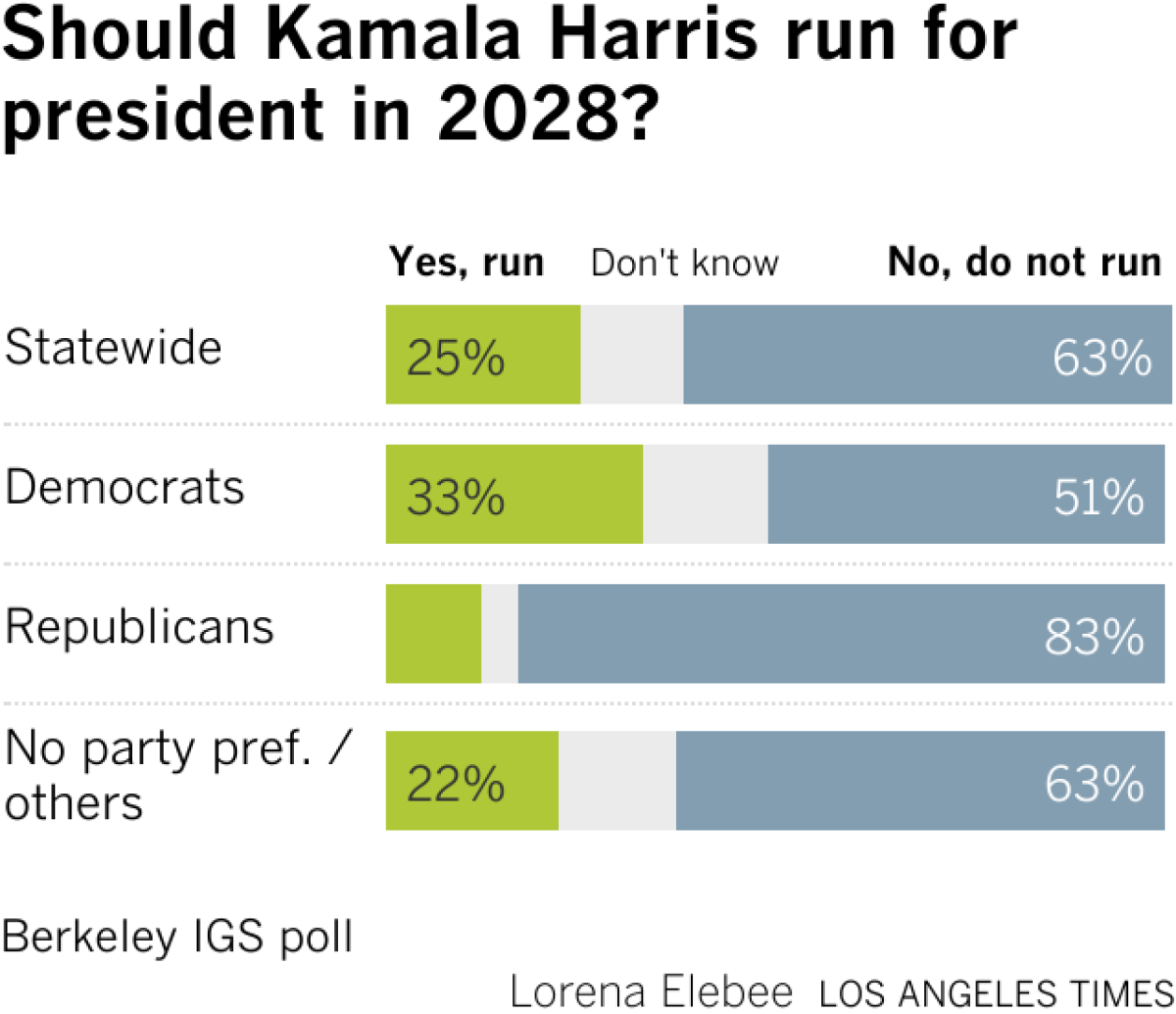
Roughly 45% of the state’s registered voters said they were very or somewhat enthusiastic about Newsom running, compared with 36% who expressed a similar sentiment about Harris. Additionally, nearly two-thirds of registered voters and 51% of Democrats said Harris should not run for president again after two unsuccessful White House bids — in the primary in 2020 and in the general election in 2024.
“She lost, which is always a negative when you’re trying to run again,” DiCamillo said. “It’s interesting that even after Harris bowed out of the governor’s race, most Californians don’t really think she should run for president.”
While he described Newsom’s support as a “mixed bag” among the state’s registered voters, DiCamillo pointed to his strength among Democrats. Nearly 7 of 10 registered Democratic voters in the state said they are very or somewhat enthusiastic about Newsom running for president, compared with 54% who expressed similar feelings about Harris.
The poll took place during a tumultuous period as Trump’s far-right policies begin to hit their stride.
Drastic cuts to healthcare, nutrition, reproductive rights and other federal safety-net programs are expected to disproportionately affect Californians. The Trump administration‘s aggressive immigration raids in Los Angeles and across the state and country have caused the nation’s partisan divide to widen, driven by the president’s decision to deploy the military and target all undocumented immigrants, including law-abiding workers. Higher-education institutions across the nation have been targeted by the Trump administration, including UCLA, which is being threatened with a $1-billion fine.
Californians were surveyed shortly before Democratic state lawmakers, trying to fight the Trump administration’s agenda, voted Thursday to call a special election in November to redraw the state’s congressional districts. The action was taken to counter gerrymandering efforts in Texas and other GOP-led states as both parties fight for control of Congress in next year’s midterm elections.
The Berkeley IGS poll surveyed 4,950 California registered voters online in English and Spanish from Aug. 11 to 17. The results are estimated to have a margin of error of 2 percentage points in either direction in the overall sample, and larger numbers for subgroups.
It was not passion that pushed Rahimat Ola* into the medical field. She had dreamed of becoming a writer, but her parents decided they wanted her to be a medical doctor because that was where the money was. After three years, from 2011 to 2013, of failed attempts to get into medical school, she settled for a degree in science laboratory technology with a speciality in microbiology. She took that option because it was the closest to her parents’ dream.
But her story was not a tragedy, because she soon became interested in it and started nursing another dream of becoming a medical researcher.
“I wanted to make so many contributions to the world through medical research and just help people,” she told HumAngle. “I rewrote the exam again and got admission to study nursing, but I didn’t take it because I had already fallen in love with medical research.”
During her Student Industrial Work Experience Scheme (SIWES) placement at a clinic, Rahimat’s dedication was such that she continued to volunteer even after the official programme ended. It was during this period that she was involved in an accident that gravely affected her.
“There was this patient who obviously looked sick, but he did not mention he was afraid of needles, so while trying to take his blood sample, he started struggling immediately. The needle pricked him, and as a result, I got pricked too,” she recounted.
Rahimat reported the incident to her senior colleagues immediately, and they asked her to wash her hands. At first, she thought little of it, until the test results for the patient came back showing he had Hepatitis C, a bloodborne virus transmissible through blood.
She tested for the virus after three months, then six months, and a year later, all came back negative. But soon afterwards, she began to notice symptoms, such as cramps and skin sensitivity. The doctors she consulted insisted everything was fine until her mother went back there with her and kept pushing for more tests. It was then that the result returned positive.
What followed was not only a medical battle but a social one. After she disclosed her condition to the head of the lab, believing it was the right step since she had contracted it at work, her medical information leaked. Stigma soon crept in, with rumours and insinuations circulating among her colleagues. “One of the lab scientists who once made romantic advances towards me started to make sexual insinuations,” she said.
Even after she explained that her doctors said that the earlier negative results might have been due to low viral load at the time of infection, some colleagues refused to believe she had contracted the infection in their lab.
Rahimat said that the stigma and gossip at her workplace had a serious impact on her.
Such disinformation is a common tactic used to distort, dismiss, and distract to stifle the voices of people, especially women. Gender disinformation is particularly widespread and perpetuates a culture of silence and shame, and also creates room for misogynistic tendencies to thrive. In Nigeria’s healthcare sector, where women make up about 60 per cent of the workforce sector, these dynamics are especially pronounced.
For Rahimat, the whispers and innuendos carried an old, familiar sting. Long before her diagnosis, she faced unwanted sexual advances from some lecturers at a medical school in northern Nigeria.
A survey of over 30,000 tertiary education students in Nigeria revealed that about 37 per cent of the respondents have experienced a form of sexual violence, with female students reporting twice as many incidents as their male counterparts.
“I knew it would have been worse if my father had not been a lecturer in another faculty in the same school. The moment they learned that, they left me alone, but some persisted,” she said.
One lecturer, she recalled, sexually harassed her throughout her four years in school. By her final year, while she worked on her thesis, the harassment turned into victimisation.
“He promised me he was going to disgrace me during my thesis defence, and he attempted it. During the defence, before any other lecturers could speak up, he started asking questions he thought I could not answer, but unfortunately for him, I answered the first two and told him the last question was beyond the scope of my study and would research more,” she said.
At times, even women lecturers blamed her for the harassment, suggesting she did not wear her hijab “properly” for a Muslim, even though the university was not a religious institution.
After graduating, Rahimat hoped such experiences were behind her. But during her National Youth Service in 2019, while working at a university lab in Oyo State, southwestern Nigeria, she faced yet another round of gender prejudice. At first, everything went smoothly, but seven months into her one-year service, the head of the lab started to make sexist remarks, claiming women were lazy and that he preferred male lab technicians.
Illustration: Akila Jibrin/HumAngle
Research shows that deep-seated beliefs about gender roles in work environments add to the systemic barriers that make it challenging for women in the workforce.
Rahimat said she would simply ignore those comments and focus on her job. This shift in her manager’s attitude coincided with the arrival of another male corps member in their team. Tension grew after her new colleague found out that her ₦30,000 stipend was higher than what he received. The school did not recognise him as a lab technician, so he earned only the extra ₦6,000 paid by the state government to corps members.
Rahimat explained to him that the extra ₦30,000 was paid to her directly by the school, not the laboratory, and that another colleague in the same role as hers was receiving the same amount. Still, the explanation did little to ease the resentment. Soon, the male colleague began spreading rumours that she was being paid more because of personal connections.
The rumours got so serious that Rahimat was summoned to the administrative office.
“I could remember, the man there said to me that if I wanted to do ‘stuff,’ I should not have done it that obviously. I told him I did not understand what he was saying, and he started to backtrack. I told them that whatever issue there was with the payment was their fault and it had nothing to do with me. Apparently, by ‘stuff’, they meant I had seduced someone to get favours, when in reality I had never even met anyone connected to the organisation before I was posted .”
Her service year was her first time in Oyo, as she grew up in northern Nigeria. She had moved there alone and did not know anyone, like most corps members.
Following the administrative summons, she was instructed to refund the extra amount she was being paid. She asked them to put the instruction in writing, and that was when they let her be. At the end of that month, the management announced that she and the male colleague would be transferred to the university’s science laboratory department, where they would work as teaching assistants.
However, Rahimat soon learnt that she was the only one who was reposted, and the male corps member was made to retain her position, a move she suspected had been the plan all along.
She felt out of place in her new role and believed the lingering rumours affected how she was treated, but eventually, colleagues began to warm up to her. However, she did not receive payments, as the management claimed they were deducting her “overpayment”.
“I felt hopeless and discouraged,” she recounted. “I felt like a nobody in the system, and it bothered me that I couldn’t change the system. It felt like it was not a safe space for me to be, and I did not want to deal with the medical field anymore.”
Determined not to give up, Rahimat attempted to start her postgraduate studies to pursue her dream of becoming a medical researcher. However, when her sister fell sick with cancer, she became her sister’s primary caregiver, putting her ambitions on hold.
This rerouted her career path. She took a job as an editor at a publishing house and sold books on the side to support her sister’s medical bills. In 2021, she started a psychology degree.
Now 29, Rahimat said she is content with her writing career and free from the complications of being a woman in the medical field.
‘Not so casual’ misogyny
Rahimat is one of many women in medicine who have faced gender discrimination at work. Janet Adam*, a medical doctor in the country’s North West, initially thought she had escaped much of it, until she examined her career more closely and realised that these experiences were normalised.
For women doctors in Nigeria like Janet, this discrimination often manifests through sociocultural biases, lower pay, and a lack of professional respect. Patients and their relatives sometimes refuse to recognise women as doctors, addressing them as nurses even after being corrected. “I have had several encounters,” she said. “I am a very vocal person, and I have actually changed it for patients.”
According to Eunice Thompson, a labour lawyer and HR and compliance expert, such behaviour can be more than just disrespect; it can be a workplace rights violation.
“Women can seek justice when they experience harassment, abuse, or injustice in the workplace,” she said. “In the course of the work I do, I noticed bullying, verbal abuse, and harassment are a common experience that women go through, and this is a violation of their right to dignity and a threat to their mental health, safety, and career.”
The lawyer advised women to document incidents by keeping a private log of events using screenshots or recordings on their phones, keeping track of the dates and who was present during the event, and if the facility has a HR professional or a complaint channel, they should utilise it even if they do not trust the system, as submitting it in writing is a form of documentation itself. She added that they should request an acknowledgement of the receipt of the complaint.
Janet believes much of the treatment she has faced stems from her gender, noting that male colleagues rarely endure the same. The pattern, she says, extends to women in other departments, like administrative workers and sometimes even to female patients.
Sometimes, this misogyny for female doctors translates into patients dismissing their diagnosis or professional advice and seeking a second opinion from a man, she explained. “Even if the male doctors asked if you [referring to a female doctor] didn’t inform them beforehand, they would say you did, but [they] still needed to confirm,” she told HumAngle.
The disrespect also comes from colleagues. During a ward round early in her career, she asked in Hausa about “the boy” usually present by a teenage patient’s bedside. A senior male colleague, with whom she’d had prior tension, berated her for using the word “boy,” dragging out the criticism “unnecessarily”.
“I don’t think he would have said anything if I [had] asked about the girl staying with the patient, as it is normal to see women, even doctors, being addressed as ‘ke,’ but they never address male doctors as ‘kai”,” she noted. In Hausa language, the informal ‘hey you’ can be seen as disrespectful, especially when there is a professional relationship.
Janet said she cautioned the colleague not to disrespect her in front of her patients again. The consultant present did not interfere in the matter.
Years later, the lack of professional respect she experienced from colleagues would echo in her interactions with patients’ relatives. In 2024, while working at an orthopaedic hospital in the same region, her colleagues informed her of the son of an elderly patient, who was known to throw his weight around, constantly referencing the fact that he came from Europe to take care of his sick father.
“The day I resumed work, I went to check on the patient, but the son kept interrupting me, asking unnecessary questions. I told him I could not comment because I hadn’t fully read the patient’s folder and had just come to check in,” Janet recounted.
However, he ignored her explanation and continued with the questions. When Janet turned to monitor the nurse who was taking the patient’s blood pressure, the man suddenly began to yell at her. “He accused me of being disrespectful,” she said.
He eventually asked her to leave the room. As she walked away, the patient’s son started to come menacingly close, as though about to hit her. When Janet asked him if he wanted to slap her, he demanded to know what she would do about it if he did. Due to the threat of violence, she reported the incident to her line manager, saying she would not treat the patient again.
The confrontation didn’t end there. The man followed her to the reception, continuing to shout. Frustrated, Janet said she shouted back at him, prompting him to bring out his phone to “record the disrespect”. “I slapped the phone from his hand and told him he could not aggravate me and then try to record my response,” she recounted.
It was not the first time she had felt the need to use extraordinary measures to tackle situations like that. “Even in medical school, I ensured not to tolerate things like this,” Janet said.
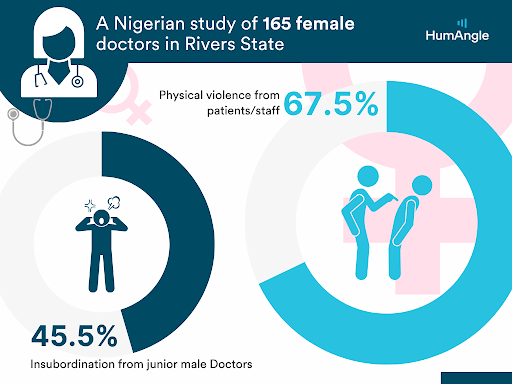
A 2023 study by the Nigerian Medical Association shows that 45.5 per cent of 165 women doctors in Nigeria’s South South have experienced physical violence from both patients and/or other staff in their work environments.
The reality of women doctors in Rivers State, South South Nigeria. Data source: The Nigerian Medical Association. Illustration: Akila Jibrin.
Twenty-five-year-old Halima Bala*, who is currently practising in Katsina, northwestern Nigeria, echoes Janet’s experience of being bullied by a patient’s relative.
“A nurse and I were the only ones on duty, and the patient’s relative, who was a big man, started shouting at both of us because there weren’t any empty bed spaces, and we had to be cautious because we didn’t know what he might do to us,” Halima recounted. “He mysteriously became calm and civil when a male colleague came to interfere. I was so upset. I even felt like I didn’t want to treat his daughter anymore, but my anger softened when I saw the state the patient was in, and I believe there is no patient I should refuse to see.”
When incidents like this happen, the hospital can either take the doctor off the case or, in more severe cases, which Halima has never witnessed personally, choose not to treat that patient. Yet, in her experience, the default approach is to side with the patient. When the hospital apologised to the man who had disrespected her instead of holding him accountable, Halima said it reinforced her understanding of how deeply entrenched and unjust misogyny can be.
However, she noted that these experiences did not deter her; if anything, they encouraged her to excel at everything she does.
Eunice said women can report such abuse to professional bodies like the Medical and Dental Council or Nursing and Midwifery Council, and if internal channels fail, they may go public or seek community support to push for accountability.
“If harassment is verbal or slanderous, people often dismiss it, but it is harmful, especially when you can prove it’s targeted and persistent. Record it and write exactly what was said, and get a trusted colleague who can serve as a witness or offer support, and you can sue for defamation too,” the labour lawyer added.
‘As a woman, you should…’
When 54-year-old Hadiza Husseini* chose to study pharmacy out of her love for helping people change for the better, she assumed it would be less consuming compared to being a doctor, hence she would be able to raise her family. While she can not recall experiencing gender discrimination and assault during her undergraduate studies, Hadiza said she came face-to-face with the challenge after she gave birth to her third child.
“I had a very misogynistic boss at that time, who would constantly make sexist comments about my womanhood and motherhood. I ignored him, but one day I completely lost it. I told him to leave all the work for me that day, and he would see that my gender or baby would not stop me from doing every work that was supposed to be done,” she recalled.
He stopped bothering her afterwards.
However, the impoliteness did not end. Years after she became a chief pharmacist, making her the third in command in her department at that time, her deputy director, who was a man, turned to her after a meeting one day and asked her to clear the dirty cups they had been drinking from since she was the only woman in the room.
“I was shocked and dumbfounded and struggled to wrap my head around it,” she recounted. “Even my junior colleagues turned to stare at him. I instinctively said, ‘What?’ and he said he thought I wouldn’t mind because I was a woman and I would enjoy doing it.”
Most of the people who drank from the cups were not only younger but also much lower in rank than her, and they were all still in the room.
Since then, there have been several other acts of gender discrimination that Hadiza has challenged. “There are people in my office who call me the minister of women’s affairs because I do not allow anyone to disrespect a woman in front of me,” she noted.
Research shows that workplace conflict, which could be a product of power imbalance, gender discrimination, resource allocation, transgenerational strain, and interprofessional relationships, affects the experiences and well-being of Nigerian medical practitioners.
Illustration: Akila Jibrin/HumAngle
In Nigeria, there is no strong anti-workplace discrimination law, but there are still legal protections that are available. Eunice, the labour lawyer, noted that Chapter 42 of the Nigerian Constitution, which states that nobody should be discriminated against based on sex, even if you are the only woman in the room or team, is one of those laws.
She also cited other laws that could be useful, such as the Violence Against Persons Prohibition Act (VAPP) and the Laws of Torts, which recognise psychological abuse as a form of violence.
“The International Women’s Rights Treaty is also a powerful advocacy tool, although it has not been fully domesticated in Nigeria. However, a law is only as useful as a system that enforces it, and enforcement is weak in Nigeria,” Eunice noted. “That is why we need more legal knowledge alongside community power and support. The fact that these things are common does not make them right. Women deserve to be treated with dignity and fairness.”
Bullied yet underpaid
Globally, nursing remains a female-dominated profession, and Erica Akin* says her nine-year career has been marked by frequent bullying from both healthcare practitioners and patients alike. “Nurses on duty get blamed for every problem in the hospital, even while it is glaring that they are not at fault. If a lab scientist does not come to get a patient’s blood for investigation, or if the patient waits too long in line to see the doctor, the nurse gets blamed,” she said.
Erica, now 34, became a professional nurse in 2016 after passing her qualifying exams on her first attempt. Despite the rigorous training and pressure during her studies, she found the workplace equally challenging. She says bullying is normalised in the sector, leaving her feeling unappreciated, and it often worsens when she stands up for herself.
“It only challenges me to be smarter and more efficient at my job to avoid disrespect of any kind,” she told HumAngle, adding that she is also concerned about how nurses are significantly underpaid in the healthcare sector.
While her federal-level salary is higher than in private facilities, she believes it still undervalues nurses’ workload. “The startup salary for the [federal government’s] Consolidated Health Salary Structure (CONHESS 9) is about ₦215,000, while private hospitals may pay ₦30,000 to ₦60,000, depending on the facility,” she said.
‘Twice as hard’
“The medical system is very toxic,” Jamilat Abdulfattah, a medical practitioner who works in Kwara State, North Central Nigeria, claimed, adding that earning her white coat has not been an easy ride. “People respect male doctors more than females, and even other health workers vividly show dislike towards you because you’re a female.”
The 26-year-old sees this as a result of the general misogynistic notion that women cannot perform as well as men. Oftentimes, this makes her feel underappreciated and sometimes pushes her to work twice as hard as her male colleagues just to get appropriate respect; on some days, it means going to work early.
“I observed that my male colleagues can just slack off, and people still respect them as doctors,” she said. “As a woman, I am always on edge and pushing myself to go the extra mile so I won’t be seen as less than, and every mistake is ascribed to my gender.”
“However, I don’t let it get to me. I call out misogynistic behaviour most time. But when it’s coming from a senior colleague, I will have to endure because the hierarchical system would not allow me to do certain things, or else I can risk getting kicked out of the system. So instead, I focus on what I can control and let what I can not control go,” Jamilat told HumAngle.
She is hopeful that these irregularities will change in the future.
“Most of us plan to break the cycle of bullying,” she said.
Names marked with an asterisk (*) have been changed to protect the identities of the sources, who spoke on condition of anonymity due to fear of harassment or further discrimination. The names of the institutions where they work have also been withheld.
If the Trump administration succeeds in barring undocumented immigrants from federally funded “public benefit” programs, vulnerable children and families across California would suffer greatly, losing access to emergency shelters, vital healthcare, early education and life-saving nutritional support, according to state and local officials who filed their opposition to the changes in federal court.
The new restrictions would harm undocumented immigrants but also U.S. citizens — including the U.S.-born children of immigrants and people suffering from mental illness and homelessness who lack documentation — and put intense stress on the state’s emergency healthcare system, the officials said.
Head Start, which provides tens of thousands of children in the state with early education, healthcare and nutritional support, may have to shutter some of its programs if the new rules barring immigrants withstand a lawsuit filed by California and other liberal-led states, officials said.
In a declaration filed as part of that litigation, Maria Guadalupe Jaime-Milehan, deputy director of the child care and developmental division of the California Department of Social Services, wrote that the restrictions would have an immediate “chilling effect” on immigrant and mixed-status families seeking support, but also cause broader “ripple effects” — especially in rural California communities that rely on such programs as “a critical safety net” for vulnerable residents, but also as major employers.
“Children would lose educational, nutritional, and healthcare services. Parents or guardians may be forced to cut spending on other critical needs to fill the gaps, and some may even be forced out of work so they can care for their children,” Jaime-Milehan said.
Rural communities would see programs shutter, and family providers lose their jobs, she wrote.
Tony Thurmond, California’s superintendent of public instruction, warned in a declaration that the “chilling effect” from such rules could potentially drive away talented educators who disagree with such policies and decide to “seek other employment that does not discriminate against children and families.”
Thurmond and Jaime-Milehan were among dozens of officials in 20 states and the District of Columbia who submitted declarations in support of those states’ lawsuit challenging the Trump administration’s new rules. Six other officials from California also submitted declarations.
The lawsuit followed announcements last month from various federal agencies — including Health and Human Services, Labor, Education and Agriculture — that funding recipients would be required to begin screening out undocumented immigrants.
The announcements followed an executive order issued by President Trump in which he said his administration would “uphold the rule of law, defend against the waste of hard-earned taxpayer resources, and protect benefits for American citizens in need, including individuals with disabilities and veterans.”
Trump’s order cited the Personal Responsibility and Work Opportunity Reconciliation Act of 1996, commonly known as welfare reform, as barring noncitizens from participating in federally funded benefits programs, and criticized past administrations for providing exemptions to that law for certain “life or safety” programs — including those now being targeted for new restrictions.
The order mandated that federal agencies restrict access to benefits programs for undocumented immigrants, in part to “prevent taxpayer resources from acting as a magnet and fueling illegal immigration to the United States.”
California and the other states sued July 21, alleging the new restrictions target working mothers and their children in violation of federal law.
“We’re not talking about waste, fraud, and abuse, we’re talking about programs that deliver essential childcare, healthcare, nutrition, and education assistance, programs that have for decades been open to all,” California Atty. Gen. Rob Bonta said.
In addition to programs like Head Start, Bonta said the new restrictions threatened access to short-term shelters for homeless people, survivors of domestic violence and at-risk youth; emergency shelters for people during extreme weather; soup kitchens, community food banks and food support services for the elderly; and healthcare for people with mental illness and substance abuse issues.
The declarations are part of a motion asking the federal judge overseeing the case to issue a preliminary injunction barring the changes from taking effect while the litigation plays out.
Beth Neary, assistant director of HIV health services at the San Francisco Department of Public Health, wrote in her declaration that the new restrictions would impede healthcare services for an array of San Francisco residents experiencing homelessness — including undocumented immigrants and U.S. citizens.
“Individuals experiencing homelessness periodically lack identity and other documents that would be needed to verify their citizenship or immigration status due to frequent moves and greater risk of theft of their belongings,” she wrote.
Colleen Chawla, chief of San Mateo County Health, wrote that her organization — the county’s “safety-net” care provider — has worked for years to build up trust in immigrant communities.
“But if our clients worry that they will not be able to qualify for the care they need, or that they or members of their family face a risk of detention or deportation if they seek care, they will stop coming,” Chawla wrote. “This will exacerbate their health conditions.”
Greta S. Hansen, chief operating officer of Santa Clara County, wrote that more than 40% of her county’s residents are foreign-born and more than 60% of the county’s children have at least one foreign-born parent — among the highest rates anywhere in the country.
The administration’s changes would threaten all of them, but also everyone else in the county, she wrote.
“The cumulative effect of patients not receiving preventive care and necessary medications would likely be a strain on Santa Clara’s emergency services, which would result in increased costs to Santa Clara and could also lead to decreased capacity for emergency care across the community,” Hansen wrote.
The Trump administration has defended the new rules, including in court.
In response to the states’ motion for preliminary injunction, attorneys for the administration argued that the rule changes are squarely in line with the 1996 welfare reform law and the rights of federal agencies to enforce it.
They wrote that the notices announcing the new rules that were sent out by federal agencies “merely recognize that the breadth of benefits available to unqualified aliens is narrower than the agencies previously interpreted,” and “restore compliance with federal law and ensure that taxpayer-funded programs intended for the American people are not diverted to subsidize unqualified aliens.”
The judge presiding over the case has yet to rule on the preliminary injunction.
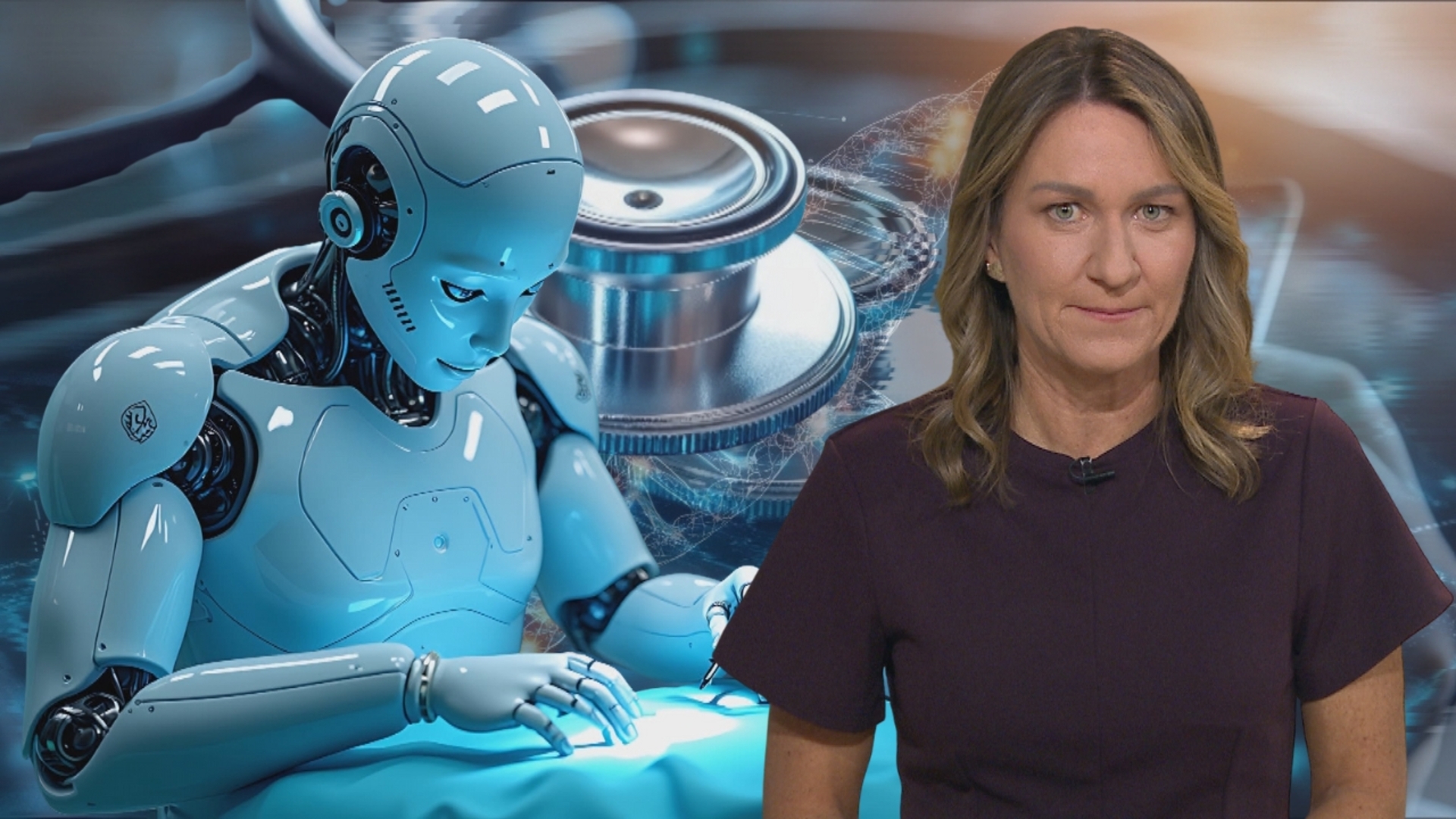
We examine how artificial intelligence is transforming physical medicine and mental health.
Artificial intelligence is being used to diagnose rare diseases and provide vital support for people dealing with anxiety and depression, taking on roles traditionally held by healthcare professionals.
But this growing reliance raises important questions: can we fully trust AI in critical health decisions? Who is accountable if mistakes are made? And how will its integration shape the future of healthcare?
Presenter: Stefanie Dekker
Guests: Andreas Michaelides – Psychologist and health tech expert
Information, in the second Trump administration, is a currency of power and fear. Last week, Atty. Gen. Pam Bondi announced sweeping subpoenas targeting physicians and medical providers who offer care for transgender youth. The aim is not to initiate prosecutions: Indeed, the legal theories upon which such prosecutions might rest are tenuous at best.
By filing these investigative demands, the government plainly hopes to chill medical providers from offering expert care. This strategy can work even if, at the end of the day, the government’s threats are hollow as a matter of law. The White House’s plainly unconstitutional attacks on law firms, for example, have substantially worked — even though the minority of firms to challenge the orders rapidly won relief.
Fortunately, the legal system is not powerless in the face of such overreaching: Federal district courts have the authority, and the obligation, to recognize that patient-physician dealings are akin to attorney-client and spousal discussions. Both of the latter benefit from judicially created privileges — or legal shields that individuals can invoke against the state’s probing. At a moment when not just gender medicine but also reproductive care more generally is in peril, federal courts can and should step in and shield intimately private medical data as well.
We suspect that many people believe that what they tell their doctors is already private. They’re right, but only sort of. There’s a federal law called HIPAA that limits what your doctor can do with the information. It says that your doctor can’t, for instance, sell your medical records to the newspaper. In 2024, the Department of Health and Human Services also issued a HIPAA “privacy rule” that heightened protections for reproductive healthcare information. (Last month, a federal district court in Texas declared the rule unconstitutional — so its future is uncertain.)
Even with the privacy rule, however, HIPAA hides a gaping hole: It allows disclosures “required by law.” And the law explicitly permits disclosures pursuant to subpoenas of all kinds — judicial, grand jury or administrative — including those issued by Bondi. So if the Justice Department subpoenas your intimate and sensitive healthcare information, HIPAA won’t stop that.
In previous academic work, we’ve urged Congress and state legislatures to fill this gap. Blue states have acted to curtail cooperation with other states — but there’s a limit to what states can do when the federal government demands information.
Yet there remains one entity that can, and should, act immediately to shield reproductive healthcare information: the same federal district courts that have been at the forefront of pushing back on the Trump administration’s many illegal and constitutional actions. We think federal courts should extend existing “privileges,” as evidentiary shields are called, to encompass both records of gender-affirming and transgender medical care, and also records of reproductive care more generally.
A privilege not only bars protected information from being admitted into evidence at trial, but also blocks subpoenas, warrants and other court orders.
Federal district courts have a general power to create privileges, and they often do so when people already have a reasonable expectation that their conversations will not be disclosed. Most people have heard of the attorney-client privilege, which means that you can confide in your lawyer without worrying that what you say will end up being used in court. But privileges can apply to all sorts of other information as well: what you tell your spouse, what you tell your spiritual advisor and even highway safety data that your state reports to the feds in exchange for funding. Existing court-created privileges protect not only attorney-client but also executive-branch communications.
Federal courts should recognize a privilege for doctor-patient communications in gender and reproductive medicine. They could do so if one of the physicians subpoenaed recently goes to court. The protection they seek is simply an extension of widely recognized legal principles and expectations of privacy. Federal courts already have recognized a privilege for patient communications with psychotherapists, and many state courts also offer privilege protections for broader doctor-patient communications.
Importantly, it is the job of federal district courts to craft evidence-related rules. After all, these are the judges who are closest to litigants and the mechanics of evidence protection. District courts don’t need to wait around for the Supreme Court to act on this, because the Federal Rules of Evidence left privileges to common law development in the district courts. And under the well-established balancing test that lower federal courts should follow when they create new privileges, we think our proposed privilege is an easy case: It serves a public purpose and protects what should be recognized as a valued interest of “transcendent importance” — privacy for our most intimate medical care.
The case for recognizing the privilege in respect to the recent subpoenas is especially strong: The attorney general is seeking to chill physicians from providing advice that is protected by the 1st Amendment and care that is guaranteed by federal statutes. Such subpoenas are directly at odds with the rule of law.
Today, it is trans kids; tomorrow, it will be people seeking an abortion or contraception. We should not have to wait for the federal government to go this far before our privacy gets the shield that it deserves.
Aziz Huq and Rebecca Wexler are professors of law at the University of Chicago Law School and Columbia Law School, respectively.
Save yourself the bother and just get ticked off now: A new poll shows that most people will be unhappy regardless of how the U.S. Supreme Court rules in its much-anticipated decision on the nation’s sweeping healthcare law.
The survey by the Pew Research Center found that regardless of whether the law is upheld, struck down or kept intact except for its “individual mandate,” fewer than half those asked would be happy with the outcome.
Not surprisingly, the poll found opinions split along partisan lines: most Democrats would be pleased if the law, President Obama’s signature domestic achievement, is allowed to stand. Most Republicans would be happy if the law is nullified.
The most closely watched group, political independents, tilted against the healthcare act. Half said they would be happy if the law was overturned, while 35% would be happy to see it upheld.
The justices issued their latest set of decisions Monday morning and the healthcare ruling was not among them. There is a chance the opinion, arguably the most consequential of the current Supreme Court term, will be issued on Thursday. Most court watchers, however, expect the decision to come sometime next week.
Overall, by a 48% to 43% margin, most of those surveyed continued to oppose the healthcare bill, though most do not have a particularly good understanding of its provisions. Only 18% said they understood the law very well, while just about half said they understood it somewhat. Nearly a third said they didn’t understand it too well or not well at all.
One explanation for the opposition could be the barrage of negative advertising surrounding the legislation. As earlier noted, critics of the law have outspent supporters more than 3 to 1 in paid TV advertising.
The Pew survey was conducted nationally June 7-17 among 2,013 adults and has a margin of error of plus or minus 2.5 percentage points.
Covered California, the state’s Affordable Care Act health insurance marketplace, estimates that as many as 660,000 of the roughly 2 million people in the program will either be stripped of coverage or drop out due to increased cost and the onerous new mandates to stay enrolled. Those who do stay could be hit with an average monthly premium increase of up to 66%.
This is Phil Willon, the L.A. Times California politics editor, filling in for columnist George Skelton this week.
To find out more about how the millions of Californians who rely on Covered California for health insurance will be affected by Trump’s megabill, I spoke with Jessica Altman, the organization’s executive director.
We spoke on Thursday, while the Republican-led U.S. House of Representatives was voting to approve the reconciliation legislation. According to estimates by the nonpartisan Congressional Budget Office, the package will lead to 11.8 million more people going without health insurance nationwide over the next decade.
Price increase imminent
Covered California serves as a marketplace exchange for state residents seeking healthcare insurance under the federal Affordable Care Act, widely known as Obamacare, allowing them to select from name-brand insurance providers and choose from a variety of coverage plans.
“A quarter of the people we cover are sole proprietors. That’s everything from mom-and-pop Etsy shops to a consultant, a highly educated tech worker in San Francisco doing contract work. We really have that full spectrum,” Altman said.
Covered California also serves as a health insurance sanctuary for residents whose income rises enough for them to lose eligiblity for Medi-Cal, as Medicaid is known in California, or those who work for companies that don’t provide benefits.
The current cost for basic coverage ranges from $0 a month for individuals earning around $21,000 — just above the income eligibility for Medi-Cal — to 8.5% of the income of people making $75,000 or more, Altman said.
Those subsidies were not renewed in the Trump megabill. In theory, the Republican-led Congress could remedy that before the end of the year but, given that Trump spent most of his first term in office trying to repeal the Affordable Care Act, the odds of that appear slim.
“We have many, many people paying less than $10 a month for their health insurance. We’re going to lose that price for sure,” Altman said. “We also have people, that person making $75,000 a year … they’re going to lose all of their tax credits and potentially pay hundreds more a month.”
And that price increase will start to hit home in four months, when Covered California’s open enrollment signup period begins for 2026.
Thousands of Californians will drop their coverage because they can no longer afford the expense, Altman predicts.
“This is a moment where Americans and Californians are so financially strained: Their rent, their food, their gas, their child care, all of their transportation, all of these things,” Altman said. “They are not in a position today where they feel like any of those costs can rise by 66%.”
Altman said the governor and California Legislature budgeted an additional $190 million for Covered California, which hopefully will help reduce the number of residents who will lose their healthcare coverage. But, she said, it’s nowhere near enough to make up for the federal cuts.
Targeting legal immigrants and ‘Dreamers’
Approximately 112,000 lawful immigrants in California also will be stripped of premium tax credits and cost-sharing support, essentially pushing health coverage out of financial reach, she said. That includes immigrant groups that have been eligible for assistance for years, including those with work and student visas, refugees, asylees and victims of human trafficking.
“They are limiting it so only green card holders and a couple of very nuanced categories of certain Cuban immigrants and certain immigrants from Pacific Island nations can get financial assistance,” Altman said.
Immigrants who grew up in the United States after being brought here illegally as children, a group known as “Dreamers,” will be stripped of their eligibility, Altman said.
Thousands more Californians likely will drop coverage because of new burdensome verification requirements, including increased tax filings, and bureaucratic hurdles that must be overcome to maintain eligibility.
Altman said that impact will be exacerbated by the tens of thousands of Californians expected to lose their medical insurance they secured through Covered California. Medical facilities received higher compensation to care for patients who secured health insurance through Covered California than they do for patients on Medi-Cal. And hospitals and clinics will now take an even greater financial hit for caring for Californians with no health insurance, raising healthcare costs for everyone else.
“We know people will get less healthcare. They will not get their preventive care, they will not get their primary care at the rates that they do when they’re covered,” Altman said. “But when they really need care, they’re going to go get it. They’re going to get it at the emergency room, and our system is going to pay for it anyway.”
United States President Donald Trump’s signature piece of budget legislation, the “One Big Beautiful Bill”, will likely raise healthcare costs, experts have said. While the Medicaid cuts will directly impact those who depend on the programme, the consequences will extend to others as well.
The 869-page bill, which includes roughly $1 trillion in cuts to Medicaid over the next decade, passed in the House along party lines, with only two Republicans – Representatives Thomas Massie of Kentucky and Brian Fitzpatrick of Pennsylvania – breaking ranks. It will be signed into law by Trump on Friday.
In addition to patients, Medicaid funds also help financially strapped hospitals and other healthcare facilities, and the cuts could lead to their closures.
Apart from this, almost 12 million people could lose health insurance by 2034 due to reductions to both Medicaid and the Affordable Care Act marketplace, according to a Congressional Budget Office analysis.
Experts warn the new law will drive up costs elsewhere in the system. Patients may face higher out-of-pocket expenses, while hospitals could be forced to lower the quality of care, raise prices, or close entirely due to the financial strain.
“There is the mistaken belief that cuts in Medicaid will only affect those on Medicaid. Many hospitals, clinics, and healthcare organisations depend on Medicaid funding for their operations. Therefore, cuts in Medicaid can adversely affect the types and quality of services they provide,” Bruce Y Lee, professor of health policy at the CUNY Graduate School of Public Health and Health Policy, told Al Jazeera.
“In fact, a number of healthcare organisations depend so heavily on Medicaid funding that they could go out of business with significant cuts.”
The cuts would hit rural hospitals hard, according to an analysis from the National Rural Hospital Association (NRHA). About 20 percent of the US population lives in rural areas, where Medicaid covers one in four adults, a higher share than in urban areas, and plays a large part in financing healthcare services.
The cuts are expected to result in a 20 percent reduction in funding for rural hospitals in half of all states.
That will hurt patients like Martha Previte and her partner Jim Earl, who live in rural Maine. Both have type 1 diabetes and rely on regular hospital visits for a range of procedures, including blood tests and kidney treatment.
“I fear that these cuts are going to close hospitals that we rely on to get care, and we’re not going to have anywhere to go,” Previte told Al Jazeera.
This bill could result in as many as 338 hospitals closing around the US. There are already nearly 800 hospitals that are facing financial hardship.
“Our goal is to help ensure hospitals can remain open for their communities, and people can get the care they need when they need it. Our nation’s health and economic future depend on it,” the American Hospital Association said in a statement condemning the bill’s passage and calling it “an extremely disappointing and very difficult day for health care in America”.
Those that stay open could result in cuts to essential care like chemotherapy and behavioural health services.
The bill does include $50bn for rural hospitals to offset the additional financial strain they will face. But because of cuts to Medicaid, that funding will not make enough of a dent to keep healthcare costs from rising and healthcare facilities from shuttering.
Analysis from the Kaiser Family Foundation found that Medicaid cuts would still lead to a drop of $155bn in federal Medicaid spending on rural hospitals over the next 10 years.
“While the President promised to lower costs for Americans, this bill is set to spike premiums and other healthcare costs,” Elizabeth Pancotti, managing director of policy and advocacy at the Groundwork Collaborative, told Al Jazeera.
Rural hospitals in the state of Missouri will be the hardest hit and are expected to lose an average of 29 percent of Medicaid funding. While Missouri’s Senator Josh Hawley, in a May op-ed in the New York Times, said cuts to Medicaid would be “politically suicidal”, he and his fellow Missouri senator, Republican Eric Schmitt, voted in support of the bill before it moved to the House of Representatives on Tuesday.
The cuts are also expected to affect nursing homes disproportionately in urban areas, according to an analysis from Brown University School of Public Health, which forecast that 579 nursing homes could shutter. Those at highest risk have a Medicaid payer share greater than 85 percent. It was found that the Medicaid cuts overwhelmingly affected nursing homes in California, Georgia, Illinois and Texas.
Looming Medicare changes
Medicaid is not the only healthcare programme seeing cuts. While Medicaid is intended for those who are low-income, Medicare covers healthcare for those 65 and older, as well as some others who have disabilities. Some patients, like Previte, receive both.
“Medicare is my primary insurer, and Medicaid picks up what Medicare does not cover. I am a type 1 insulin-dependent diabetic of 41 years with serious complications. Medicare covered my recent hospitalisation and upcoming outpatient procedures,” Previte told Al Jazeera.
The Republican bill could also indirectly lead to cuts in Medicare services because of the statutory Pay‑As‑You‑Go Act of 2010. Under this, the White House’s Office of Management and Budget is required to keep a “scorecard” to track net increases to the deficit, with a goal to “eliminate the overage”.
Because of that, the programme may not get all of the money allocated to it, a potential $490bn loss in access to funds over the next decade, according to the Congressional Budget Office, affecting coverage for people who rely on Medicare.
“The whole thing [the tax bill] is a stark abandonment of human social responsibility,” Previte’s partner Earl said.
Affordable Care Act changes
The upcoming law also makes significant changes to the Affordable Care Act, otherwise known as Obamacare. It shortens the annual enrollment period for healthcare coverage by about a month and drives up premium costs for those who need it.
According to analysis from the Kaiser Family Foundation, insurance premium prices could increase on average by $1,296 a year.
Those who get their healthcare coverage through the exchange will also need to annually update their personal information, which includes income and immigration status, rather than being enrolled automatically.
The changes will cause a strain on the small business economy. Last year, as many as 3.3 million self-employed individuals and small business owners relied on the marketplace for health insurance.
“If you’re a young business owner, already stretched thin by housing costs, child care bills, and health premiums, this bill just made your future harder,” Richard Trent, executive director of Main Street Alliance, an advocacy group for small businesses, said in a statement.
Former President Barack Obama, in a post on X, weighed in as the bill strips parts of his signature policy, a key part of his legacy.
“It will increase costs and hurt working class families for generations to come,” the former president said in a post before the bill’s passage.
“This will be another branch of a limb of a disastrous tree. I’m concerned about what this means for our future care. The thing with diabetes, like many ailments, they’re livable if they’re treated properly. You can live a long, happy, healthy life, but when you’re deprived of healthcare, maintenance-of-health care, and things like that, then a whole Pandora’s box of disasters can happen to your health,” Earl added.
WASHINGTON — After an overnight session and hours of floor debate, the House voted Thursday to approve the “Big Beautiful Bill” — clearing its final hurdle in a landmark achievement for President Trump, who wrangled Republican lawmakers to pass the most expensive legislation in history by the Fourth of July.
The 218 to 214 vote, which saw two Republican members side with the Democrats in opposition, was delayed by a record-breaking speech on the House floor by Minority Leader Hakeem Jeffries that lasted eight hours and 44 minutes. “I’m going to take my time,” Jeffries said before launching into a marathon excoriation of the legislation, its Medicaid cuts and its Republican backers. “Shame on this institution if this bill passes.”
The bill encompasses Trump’s domestic agenda, extending tax breaks to millions of American households and businesses that are projected to add trillions to the national debt. The legislation also introduces new tax relief for senior citizens, tip and overtime workers, and new parents.
To offset a fraction of those costs, Republicans approved new barriers to access for Medicaid and cut funding streams under the Affordable Care Act, placing the healthcare of nearly 12 million in jeopardy over the next decade, according to the nonpartisan Congressional Budget Office. Funding for the Supplemental Nutrition Assistance Program, which provides food stamps, was also cut.
It has been a controversial bill within the Republican Party ever since it was conceived at the beginning of Trump’s second term, with fiscal hawks decrying its record contributions to annual deficits, and moderate Republicans fearing its cuts to healthcare would come back to haunt them in future elections.
Speaking with reporters after the vote, senior White House officials said Trump was the “omnipresent force behind the legislation,” crediting his personal relationships with lawmakers on the Hill for its ultimate success.
“I’ve lost count of the number of meetings the president has had,” one White House official said, adding that the bill “satisfies virtually every campaign promise the president made.”
Karoline Leavitt, the White House press secretary, said that Republicans defied the “doubters and the panicans” to secure passage of legislation that would “add funding for at least 1 million deportations per year.”
Beyond tax relief and healthcare cuts, the bill increases defense spending and adds a historic $150 billion to fund border security and mass deportations, exponentially increasing the budget of Immigration and Customs Enforcement — a fund larger than many national armies.
The president, Leavitt said, would host a “big, beautiful signing ceremony” Friday at 5 p.m. Eastern, marked by fireworks on the National Mall celebrating Independence Day — a deadline he imposed on the Republican caucus to secure passage of the legislation.
It also includes a host of parochial provisions. The bill provides $1 billion for security, planning and other costs for the 2028 Olympics in Los Angeles, and $30 million for the construction of a sculpture-laden “American Garden of Heroes” to be built at an undetermined location.
In total, the Congressional Budget Office projects the bill could add up to $3.3 trillion to the debt by 2034. Republicans dispute the figure as inflated, arguing the CBO assumes status economic growth, while still other groups say the projection is conservative.
In a statement after the vote, the Committee for a Responsible Federal Budget, which has advocated fiscal responsibility for decades, warned the bill “would add more than $4 trillion to the debt, accelerate the insolvency of Social Security and Medicare, and leave us even more vulnerable to the whims of the Treasury markets.”
“In a massive fiscal capitulation, Congress has passed the single most expensive, dishonest, and reckless budget reconciliation bill ever — and, it comes amidst an already alarming fiscal situation,” the group said. “Never before has a piece of legislation been jammed through with such disregard for our fiscal outlook, the budget process, and the impact it will have on the well-being of the country and future generations.”
And yet, despite issuing scathing criticisms of the Senate language for its historic contributions to the debt, opposition from the House Freedom Caucus, also founded to advocate for fiscal responsibility, all but melted away in the early hours of Thursday under intense pressure from the White House.
Several of the Medicaid provisions kick in only after the 2026 midterms, buying Republicans time to sell the bill without facing its real-world consequences before the next election. But Democrats are already campaigning against the legislation as the greatest attack on healthcare since Republicans tried to repeal the Affordable Care Act in 2017, which prompted a Democratic wave in midterms the following year.
The legislation introduces a work requirement for Medicaid enrollment that will require extensive new paperwork for applicants, and restricts state taxes on healthcare providers, known as the “provider tax,” an essential tool for many states in their efforts to supplement Medicaid funding.
Several Republican lawmakers fear that provision could have devastating effects on rural hospitals. The Senate added a rural hospital fund to the bill to help mitigate some of the impacts of the funding cuts.
The bill also rolls back green energy tax credits that have fueled an entire manufacturing workforce in wind and solar energy in states across the country.
The bill passed through the Senate despite bipartisan opposition, with three Republicans joining Democrats to vote against it. House approval of the Senate text Thursday morning occurred barely 24 hours after the upper chamber’s vote.
On Wednesday night, a number of House Republican lawmakers had said openly they would not support a rushed process to approve the bill. But a floor vote on debate rules kept open by House Speaker Mike Johnson throughout the night kept conversations active, and ultimately swayed the holdouts.
Two Republican House members, Reps. Brian Fitzpatrick of Pennsylvania and Thomas Massie of Kentucky, voted against the final bill, citing its effects to the healthcare system and to the national debt, respectively.
“What a great night it was,” Trump wrote on his Truth Social platform before the final vote. “One of the most consequential Bills ever. The USA is the ‘HOTTEST’ Country in the World, by far!!!”
In the call with reporters, one White House official also credited Vice President JD Vance for his efforts to secure a victory on the legislation, noting his huddle hours before a final Senate vote on Tuesday with Republican Sen. Lisa Murkowski of Alaska, a lawmaker who secured exceptional carve-outs for her state in the bill and yet still expressed disappointment with its harshest provisions after voting to approve it.
Democrats will welcome the vice president receiving credit. Several expressed hope to The Times they can tie any successor of Trump’s to unpopular healthcare cuts in 2028.
WASHINGTON — There’s no filibuster in the House, but Democratic leader Hakeem Jeffries essentially conducted one anyway.
Jeffries held the House floor for more than eight hours Thursday, taking his “sweet time” with a marathon floor speech that delayed passage of Republicans’ massive tax and spending cuts legislation and gave his minority party a lengthy spotlight to excoriate what he called an “immoral” bill.
As Democratic leader, Jeffries can speak for as long as he wants during debate on legislation — hence its nickname on Capitol Hill, the “magic minute,” that lasts as long as leaders are speaking.
He began the speech at 4:53 a.m. EDT and finished at 1:37 p.m. EDT, 8 hours, 44 minutes later, breaking the record set by then-Rep. Kevin McCarthy (R-Bakersfield) in 2021, when he was the GOP leader. McCarthy spoke for 8 hours, 32 minutes when he angrily criticized Democrats’ “Build Back Better” legislation, breaking a record set by Rep. Nancy Pelosi (D-San Francisco), when she spoke about immigration for 8 hours, 7 minutes in 2018.
“I feel an obligation, Mr. Speaker, to stand on this House floor and take my sweet time,” Jeffries said as he opened.
The speech pushed a final vote on Republican President Trump’s tax bill, initially expected in the early morning, into the daylight hours. The New York Democrat used the time to criticize the bill’s healthcare and food aid cuts, tax breaks for the wealthy and rollbacks to renewable energy programs, among other parts of the bill that Democrats decry.
He also killed time by riffing on hip-hop, King George III and his own life story, among other diversions. He called out Republicans who have voiced concerns about the bill, read stories from people concerned about their health care from those GOP lawmakers’ districts and praised his own members, some of whom sat behind him and cheered, clapped, laughed and joined hands.
“This reckless Republican budget is an immoral document, and that is why I stand here on the floor of the House of Representatives with my colleagues in the House Democratic caucus to stand up and push back against it with everything we have,” Jeffries said.
He ended the speech in the cadence of a Sunday sermon, with most of the Democratic caucus in a tight huddle around him. One colleague called out, “Bring it home, Hakeem!”
“We don’t work for President Donald Trump,” Jeffries said, as a handful of Republicans across the aisle sat silent and occasionally snickered at the leader as he kept talking.
He invoked the late John Lewis, a civil rights activist in the 1960s and longtime Democratic congressman from Georgia. “Get into good trouble, necessary trouble,” Jeffries said. “We’re going to press on until victory is won.”
Jeffries sneaked small bites of food and drank liquids to boost his energy, but did not leave the chamber or his podium. The speech would be over if he did.
Democrats were powerless to stop the huge bill, which Republicans are passing by using an obscure budget procedure that bypasses the Senate filibuster. So they were using the powers they do have, mostly to delay. In the Senate, Democratic leader Chuck Schumer of New York forced Senate clerks to read the bill for almost 16 hours over the weekend.
Sen. Cory Booker (D-N.J.) similarly gained attention in April when he spoke for more than 25 hours on the Senate floor about the first months of Trump’s presidency and broke the record for the longest continuous Senate floor speech in the chamber’s history. Booker was assisted by fellow Democrats who gave him a break from speaking by asking him questions on the Senate floor, but Jeffries’ “magic minute” did not allow for any interaction with other members.
Republicans who were sitting on the floor when Jeffries started trickled out, leaving half the chamber empty. When the speech was over, House Ways and Means Committee Chairman Jason Smith (R-Mo.) called it “a bunch of hogwash.”
The speech “will not change the outcome that you will see very shortly,” Smith said.
After the bill passed, House Majority Leader Steve Scalise said that Democrats “wanted to speak for hours and hours and break records because they wanted to stand in the way of history.”
Jalonick writes for the Associated Press. A.P. writers Matt Brown, Kevin Freking, Lisa Mascaro and Leah Askrinam contributed to this report.
Protesters railed on Tuesday against an Orange County congresswoman who could be a critical vote on President Trump’s proposal to cut more than $1 trillion in federal dollars that helped pay for healthcare for those in need and extend tax cuts for millions of Americans.
Trump’s proposed “One Big Beautiful Bill Act” narrowly passed the U.S. Senate hours before hundreds of people gathered in a cul-de-sac outside of the Anaheim field office of Republican Rep. Young Kim to protest those cuts. The legislation still needs to be voted on by the U.S. House of Representatives, which could happen before the end of the week.
“I don’t know why they call it beautiful, because there’s nothing about it that’s beautiful. It’s harmful, it’s reckless, and it’s cruel, and it’s going to hurt people,” said Melody Mendenhall, a nurse at UCLA who is active with the California Nurses Assn., which was among the groups that organized the protest. “Rep. Young Kim, hear our cry, hear our voices. We need our Medicaid. We cannot afford this type of reckless cuts and behavior.”
A security guard blocked the parking lot to Kim’s office and at least a half-dozen Anaheim police officers watched the protest unfold.
Several people who appeared to be Kim staffers watched the demonstration from outside the building before they dashed inside when protesters marched to the building, unsuccessfully sought to enter it and then began chanting “Shame! Shame!”
In a statement, Kim said that her door was always open to Californians in her district.
“I understand some of my constituents are concerned and know how important Medicaid services are for many in my community, which is why I voted to protect and strengthen Medicaid services for our most vulnerable citizens who truly need it,” Kim said. “I have met with many of these local healthcare advocates in recent months.”
Trump’s proposal would dramatically overhaul the nation’s tax code by making cuts approved during the president’s first term permanent, a major benefit to the corporations and the nation’s wealthy, while slashing funding for historic federal safety-net programs including Medicaid and the Supplemental Nutrition Assistance Program, which helps provide food to low-income Americans.
Roughly 15 million Californians, more than a third of the state, are on Medi-Cal, the state’s version of Medicaid, with some of the highest percentages in rural counties that supported Trump in the November election. More than half of California children receive healthcare coverage through Medi-Cal.
A version of the Republican bill was passed by the U.S. House of Representatives with Kim’s support. The U.S. Senate narrowly approved an amended version of the bill on Tuesday. The defection of three GOP senators meant Vice President JD Vance had to cast the tie-breaking vote for it to pass in that chamber.
The House and Senate will now work to reconcile their two different versions of the bill. This week was a district work week for members of Congress, but House Speaker Mike Johnson (R-Louisiana) ordered members back to Washington, D.C., for votes on the bill that could occur Wednesday or Thursday.
Republicans hope to get the legislation to President Trump’s desk for his signature by Friday, Independence Day, though there is some concern among its members about whether they will have enough votes to pass the bill because of potential defections and the united Democratic opposition.
Trump praised the passage of the bill on social media and urged House Republicans to support the Senate plan.
The proposal has caused a rift within the GOP, with and some House members have expressed reservations about the measure because of the amount it would add to the nation’s deficit and its impact on their constituents.
“I’ve been clear from the start that I will not support a final reconciliation bill that makes harmful cuts to Medicaid, puts critical funding at risk, or threatens the stability of healthcare providers” in his congressional district, Rep. David Valadao (R-Hanford) wrote on the social media site X on Sunday.
The congresswoman was en route to Washington at the time of the protest, according to a spokesperson.
Outside her Anaheim field office, protester after protester described how the bill would impact vulnerable Californians, such as disabled children, the elderly, veterans and those who would lose access to reproductive healthcare.
“The stakes have never been higher. We are living in a time when our rights are under attack,” said Emily Escobar, a public advocacy manager for Planned Parenthood of Orange and San Bernardino Counties.
She said that federal funds do not pay for abortions, but help pay for other vital healthcare, such as cancer screenings, preventative care, testing and treatment for sexually transmitted infections and access to contraception. More than one-third of Planned Parenthood’s patients nationwide reside in California.
These cuts will result in clinics being shut down, effectively reducing access to abortion, Escobar said.
“Let me make this clear, this bill is a backdoor abortion ban,” she said.
Shari Home, 73, said she and her husband were weighing how to divide their Social Security income on food, medication and medical supplies after her husband, who suffers several chronic health conditions, fell last year.
“The hospitalizations were so expensive, so we applied for and got Medi-Cal in January and food assistance, and it’s been such a lifesaver,” said the Laguna Woods resident. “Without Medi-Cal, I don’t know what we would do. Our lives would not be good. We would not have the medications that he needs.”
Michelle Del Rosario, 57, wore a button picturing her son William, 25, on her blouse. The Orange resident, one of Kim’s constituents who has previously voted for her, is the primary caregiver for her son, who has autism, epilepsy and does not speak.
Her son relies on his Medi-Cal coverage for his $5,000-a-month seizure medicine, as well as the home health support he receives, she said.
“He lives at home. He has desires, at some point, to live independently, to work, but he needs” these support services for that to happen, Del Rosario said.
SACRAMENTO — California Gov. Gavin Newsom signed on Friday a budget that pares back a number of progressive priorities, including a landmark healthcare expansion for low-income adult immigrants without legal status, to close a $12-billion deficit.
It’s the third year in a row the nation’s most populous state has been forced to slash funding or stop some of the programs championed by Democratic leaders. Lawmakers passed the budget earlier in the day following an agreement of a $321-billion spending plan between Newsom and Democratic leaders.
But the whole budget will be void if lawmakers don’t send him legislation to make it easier to build housing by Monday.
The budget avoids some of the most devastating cuts to essential safety net programs, state leaders said. They mostly relied on using state savings, borrowing from special funds and delaying payments to plug the budget hole.
“It’s balanced, it maintains substantial reserves, and it’s focused on supporting Californians,” Newsom said in a statement about the budget.
California also faces potential federal cuts to healthcare programs and broad economic uncertainty that could force even deeper cuts. Newsom in May estimated that federal policies — including on tariffs and immigration enforcement — could reduce state tax revenue by $16 billion.
“We’ve had to make some tough decisions,” Senate President Pro Tempore Mike McGuire said Friday. “I know we’re not going to please everyone, but we’re doing this without any new taxes on everyday Californians.”
Republican lawmakers said they were left out of budget negotiations. They also criticized Democrats for not doing enough to address future deficits, which could range between $17 billion to $24 billion annually.
“We’re increasing borrowing, we’re taking away from the rainy day fund, and we’re not reducing our spending,” said Republican state Sen. Tony Strickland prior to the vote. “And this budget also does nothing about affordability in California.”
Here’s a look at spending in key areas:
Healthcare
Under the budget deal, California will stop enrolling new adult patients without legal status in its state-funded healthcare program for low-income people starting 2026. The state will also implement a $30 monthly premium July 2027 for immigrants remaining on the program, including some with legal status. The premiums would apply to adults under 60 years old.
The changes to the program, known as Medi-Cal, are a scaled-back version of Newsom’s proposal in May. Still, it’s a major blow to an ambitious program started last year to help the state inch closer to a goal of universal healthcare.
Democratic state Sen. María Elena Durazo broke with her party and voted “no” on the healthcare changes, calling them a betrayal of immigrant communities.
The deal also removes $78 million in funding for mental health phone lines, including a program that served 100,000 people annually. It will eliminate funding that helps pay for dental services for low-income people in 2026 and delay implementation of legislation requiring health insurance to cover fertility services by six months to 2026.
But lawmakers also successfully pushed back on several proposed cuts from Newsom that they called “draconian.”
The deal secures funding for a program providing in-home domestic and personal care services for some low-income residents and Californians with disabilities. It also avoids cuts to Planned Parenthood.
Environment
Lawmakers agreed to let the state tap $1 billion from its cap-and-trade program to fund state firefighting efforts. The cap-and-trade program is a market-based system aimed at reducing carbon emissions. Companies have to buy credits to pollute, and that money goes into a fund lawmakers are supposed to tap for climate-related spending.
Newsom wanted to reauthorize the program through 2045, with a guarantee that $1 billion would annually go to the state’s long-delayed high-speed rail project. The budget doesn’t make that commitment, as lawmakers wanted to hash out spending plans outside of the budget process. The rail project currently receives 25% of the cap-and-trade proceeds, which is roughly $1 billion annually depending on the year.
Legislative leaders also approved funding to help transition part-time firefighters into full-time positions. Many state firefighters only work nine months each year, which lawmakers said harms the state’s ability to prevent and fight wildfires. The deal includes $10 million to increase the daily wage for incarcerated firefighters, who earn $5.80 to $10.24 a day currently.
Public safety
The budget agreement will provide $80 million to help implement a tough-on-crime initiative voters overwhelmingly approved last year. The measure makes shoplifting a felony for repeat offenders, increases penalties for some drug charges and gives judges the authority to order people with multiple drug charges into treatment.
Most of the fund, $50 million, will help counties build more behavioral health beds. Probation officers will get $15 million for pretrial services and courts will receive $20 million to support increased caseloads.
Advocates of the measure — including sheriffs, district attorneys and probation officers — said that’s not enough money. Some have estimated it would take around $400 million for the first year of the program.
Other priorities
Newsom and lawmakers agreed to raise the state’s film tax credit from $330 million to $750 million annually to boost Hollywood. The program, a priority for Newsom, will start this year and expire in 2030.
The budget provides $10 million to help support immigration legal services, including deportation defense.
But cities and counties won’t see new funding to help them address homelessness next year, which local leaders said could lead to the loss of thousands of shelter beds.
The budget also doesn’t act on Newsom’s proposal to streamline a project to create a massive underground tunnel to reroute a big part of the state’s water supply.
As many as 3.4 million Californians could lose their state Medi-Cal health insurance under the budget bill making its way through the U.S. Senate, Gov. Gavin Newsom said Friday.
Newsom said the proposed cuts to healthcare in the “one big, beautiful bill,” a cornerstone of President Trump’s second-term agenda, could force the closure of struggling rural hospitals, reduce government food assistance for those in need and drive up premiums for people who rely on Covered California, the state’s Affordable Care Act health insurance marketplace.
“This is devastating,” Newsom said. “I know that word is often overused in this line of work, but this is, in many ways, an understatement of how reckless and cruel and damaging this is.”
Medicaid provides health insurance for about 1 in 5 Americans and generally uses income, rather than employment, as a condition for enrollment.
Roughly 15 million Californians, more than a third of the state, are on Medi-Cal, the state’s version of Medicaid, with some of the highest percentages in rural counties that supported Trump in the November election. More than half of California children receive healthcare coverage through Medi-Cal.
The Senate is still debating its version of the bill. But the current version would require many Medicaid recipients to prove every six months that they work, volunteer or attend school at least 80 hours per month. States would be required to set up their work eligibility verification systems by the end of 2026, just after the midterm elections. States that do not set up those systems could lose federal Medicaid funding.
Republican House Speaker Mike Johnson told reporters last month that the aim of the policy was to encourage poor Americans to contribute and “return the dignity of work to young men who need to be out working instead of playing video games all day.”
The nonpartisan Congressional Budget Office estimated this month that the requirements would cut about $344 billion in Medicaid spending over a decade and leave 4.8 million more people uninsured.
Health policy experts warn that work requirements can lead to people who are eligible, but can’t prove it, losing their benefits.
Newsom said 5.1 million people in California would need to go through the work verification progress and about one-third would “likely” meet the requirements.
The other two-thirds would “go through the labyrinth of manual verification,” Newsom said.
He said 3 million people in California could lose coverage through the new Medicaid work requirements, and 400,000 more could lose their insurance if they were required to re-verify their eligibility every six months. Newsom said that the state’s estimate was based on the number of people who dropped off Medicaid in New Hampshire and Arkansas after those states briefly implemented their own work requirements.
Last year, California became the first state in the nation to offer healthcare to low-income undocumented immigrants. The expansion, approved by Newsom and the Democratic-led Legislature, has cost the state billions and drawn sharp criticism from Republicans.
Assembly Minority Leader James Gallagher (R-Yuba City), who has previously called on Newsom to walk back that coverage, said on social media Friday that Newsom and Democratic legislative leaders had “obliterated” the healthcare system.
Newsom’s budget proposal in May proposed substantial cuts to the healthcare program for undocumented immigrants, including freezing new enrollment in 2026, requiring adults to pay $100 monthly premiums and cutting full dental coverage.
Lawmakers ultimately agreed to require undocumented immigrant adults ages 19 to 59 to pay $30 monthly premiums beginning July 2027. Their plan adopts Newsom’s enrollment cap but gives people three months to reapply if their coverage lapses instead of immediately cutting off their eligibility. Democrats agreed to cut full dental coverage for adult immigrants who are undocumented, but delayed the change until July 1, 2026.
In Congress, the GOP bill could also pose a serious threat to 16 struggling hospitals in 14 rural counties, which received a $300-million lifeline in interest-free loans in 2023, Newsom said.
He said the Republican members of Congress in California who supported the bill and represent rural parts of California, including Central Valley Rep. David Valadao (R-Hanford) and Rep. Kevin Kiley (R-Rocklin), are “gutting an already vulnerable system.”
Some senators are pushing to change a requirement that would require states to freeze and cut by half the tax they impose on Medicaid providers, slashing a key source of funding for rural hospitals.
Michelle Baass, the director of the California Department of Health Care Services, said that change could be “fatal for the many rural and critical-access hospitals that are already financially strained.”
Newsom said in aggregate, the cuts could threaten California’s progress in reducing the share of residents without health insurance, which stands at about 6.4%.
Reporting from Washington — Judge Brett Kavanaugh on Wednesday defended his broad view of gun rights and skepticism of federal regulatory agencies, but left uncertain his position on abortion and refused to detail his views on executive power, including whether a president can be ordered to answer questions in a criminal investigation.
Facing senators during a second day of his confirmation hearing that began in the morning and stretched well into the night, President Trump’s Supreme Court nominee proved adept at giving lengthy answers without fully revealing his views on matters of controversy.
“You’re learning to filibuster,” Sen. Dianne Feinstein (D-Calif.) told him when he steered around her question on whether the president is shielded from being investigated or questioned while in office.
As the evening wore on, none of the exchanges seemed to have changed the vote count in favor of Kavanaugh’s narrow confirmation. At only one point during the hearing — faced with questions about his knowledge of emails allegedly stolen from Democratic senators during the George W. Bush administration — did the otherwise well-prepared nominee appear flustered.
On presidential power, in particular, Kavanaugh seemed to come armed with a well-honed set of responses to questions about his previous writings.
In law review articles in 1998 and 2009, Kavanaugh said the president “should be excused from some of the burdens of ordinary citizenship while serving in office” and should not be subject to investigations or questioning. The “Constitution seems to dictate” that Congress, not a special prosecutor, should investigate a president for lawbreaking, he wrote.
But when pressed repeatedly by Democrats on Wednesday, Kavanaugh contended that he has never taken a position on whether the Constitution allows for indicting or investigating a sitting president for criminal wrongdoing. He did say a president could be tried and convicted after leaving office, whether at the end of a term or because of impeachment.
“I don’t think anyone thinks of immunity” for a president, he said.
The issue has taken on new significance because Trump is caught up in special counsel Robert S. Mueller III’s investigation of Russian interference in the 2016 election and could be called to answer questions from a grand jury.
Senate Judiciary Committee Chairman Charles E. Grassley (R-Iowa), joining other Republicans in trying to help the nominee articulate his views, asked Kavanaugh “whether you have any trouble ruling against a president who appointed you.”
“You’re correct. No one is above the law in our constitutional system,” Kavanaugh said. “The executive branch is subject to the law, subject to the court system.”
Kavanaugh passed up a chance to show his independence from Trump when Sen. Jeff Flake (R-Ariz.) asked him whether he thought it was appropriate for the president to attack Atty. Gen. Jeff Sessions for his prosecutors’ indictments of two GOP congressmen — Reps. Chris Collins of New York and Duncan Hunter of Alpine — ahead of the November election. Trump said it might endanger their reelection, ignoring the serious criminal charges against the men. Kavanaugh declined to offer his opinion. He also rebuffed a request from one Democratic senator that he recuse himself from any future cases involving the Mueller investigation of Trump and his campaign.
When Feinstein asked, “Can a sitting a president be required to respond to a subpoena?” Kavanaugh would not answer. “That’s a hypothetical question,” he said. “I can’t give you an answer to a hypothetical question.”
Kavanaugh did endorse as correct the Supreme Court’s 1974 ruling in United States vs. Nixon, which required President Nixon to turn over the Watergate tapes. It was “one of the greatest moments in American judicial history,” he said.
But he refused to give a similar endorsement for the 1973 ruling in Roe vs. Wade, which established a woman’s right to abortion. Feinstein tried to get him to say whether the ruling was correct; Kavanaugh said only that it was entitled to respect as a precedent.
Most legal experts predict that Kavanaugh, if confirmed, will provide the fifth conservative vote on the court to at least restrict abortion rights, if not overturn Roe. During his campaign, Trump promised to appoint only judges who would vote to overturn the abortion ruling.
But Kavanaugh seemed eager to raise some doubts about those predictions.
“I understand the significance on the issue,” he said Wednesday. “I don’t live in a bubble. I live in the real world.”
Kavanaugh noted several times that the 1973 abortion decision had been repeatedly affirmed, and that a 1992 ruling in Planned Parenthood vs. Casey, which affirmed much of Roe, in effect created a “precedent on precedent.”
And he made an analogy to the late Chief Justice William H. Rehnquist’s decision not to overturn the so-called Miranda rights disclosure requirement for criminal suspects. Rehnquist had long opposed the Miranda ruling, but then decided it was too late to overturn it, he noted. It’s also true, however, that Rehnquist found ways to narrow the ruling’s impact.
Kavanaugh’s remarks about Roe may have been largely directed at two female Republican senators, who support abortion rights and whose votes will be key to his confirmation. Sens. Susan Collins of Maine and Lisa Murkowski of Alaska have not announced how they will vote.
But Kavanaugh gave no assurances about how he might vote, and nothing he said committed him to any particular outcome. In the past, some Supreme Court nominees have spoken about the importance of respecting precedents, and then once on the court voted to overturn them.
Feinstein, for one, seem unsatisfied. “We can’t accept vague promises from Brett Kavanaugh when women’s reproductive freedom is at stake,” she said on Twitter.
Last fall, Kavanaugh was involved in a dispute over whether a migrant teenager in Texas could be released from immigration custody to obtain an abortion. A federal judge cleared the way, but Kavanaugh wrote a 2-1 decision siding with Trump administration lawyers and blocking the abortion for up to 10 more days. The full appeals court intervened and overturned his ruling.
In dissent, Kavanaugh faulted his more liberal colleagues for wrongly creating a “new right for unlawful immigrant minors in U.S. government detention to obtain abortion on demand.”
He defended that ruling Wednesday, stressing that the girl was 17 and not yet an adult. “If she had been an adult, she would have had a right to obtain an abortion immediately,” he told Sen. Richard J. Durbin (D-Ill.).
Durbin rejected the distinction, noting that the teenager had appeared before a state judge in Texas who decided she was sufficiently mature to make the decision on her own.
On guns, Kavanaugh stuck fast to his support of a broad 2nd Amendment right to possess many types of weapons, including a semiautomatic rifle with a large magazine of ammunition.
He dissented alone in 2011 when the U.S. Court of Appeals for the District of Columbia Circuit upheld a D.C. ordinance that prohibited semiautomatic “assault weapons.”
Three years before, the Supreme Court in District of Columbia vs. Heller struck down a law prohibiting possession of a handgun at home and established a 2nd Amendment individual right for gun ownership.
Feinstein asked why Kavanaugh believed semiautomatic weapons could not be banned, when appellate judges across the country had upheld such restrictions.
“I had to follow precedent,” Kavanaugh replied. He said the late Justice Antonin Scalia said the 2nd Amendment did not protect weapons that are “dangerous and unusual,” and semiautomatic rifles are not unusual, he said. They are “widely possessed” by millions of gun owners, he said.
Kavanaugh did not back off, even when Feinstein spoke about the wave of mass shootings at schools using assault weapons. He stuck to the same position later when pressed by Democratic Sen. Richard Blumenthal of Connecticut.
On the question of presidential power, Kavanaugh said that “no one is above the law,” a standard response by nominees.
But he declined to answer questions about whether Trump could pardon himself or pardon someone in exchange for an agreement not to testify against him, saying those were “hypothetical” questions that he couldn’t answer without potentially prejudging issues that might come before the courts.
The one issue that seemed to throw the nominee came from Sen. Patrick J. Leahy (D-Vt.), who confronted him with what the senator said was evidence that a Republican staff member during George W. Bush’s administration had supplied Kavanaugh — who was then helping to confirm judges — with information that had been stolen from Democratic files. Leahy said the information detailed what the senator planned to ask nominees during confirmation hearings.
Leahy, whose emails were stolen, quizzed Kavanaugh on whether he knowingly used the stolen documents, noting that Kavanaugh was included in an email chain discussing the information. Kavanaugh said he did not recall. “I don’t really have a specific recollection of any of this,” he told lawmakers.
Leahy said later Wednesday that Grassley agreed to release documents related to the materials he said were stolen, which are now confined only to lawmakers on the committee.
Grassley’s office didn’t make the same pledge. Spokesman Taylor Foy said Grassley would “do his best to accommodate this last-minute request,” adding that waiving the classification would require input from the White House and former President Bush.
Some of the most robust exchanges came near the end from Sen. Kamala Harris (D-Calif.), who has developed a reputation for her tough questioning of Trump nominees during confirmation hearings.
Harris referred back to Kavanaugh’s remark about a “precedent on precedent” concerning Roe vs. Wade, and asked if it were not true that any five justices could overturn a precedent if they wanted.
“There’s a reason why the Supreme Court doesn’t do that,” Kavanaugh responded. “There are times” when the justices do, he said, but it’s “rare.”
She also pressed Kavanaugh on whether he had any conversations about the Mueller investigation with anyone at a law firm founded by one of the president’s lawyers. Kavanaugh avoided answering the question several times, finally saying he remembered no such conversation. A Democratic aide said that Harris’ staff was continuing to investigate the matter.
Kavanaugh was pressed repeatedly to explain his relationship with Judge Alex Kozinski, the former chief judge of the 9th Circuit Court of Appeals who retired last December after he was accused of sexually harassing female law clerks.
In 1991, Kavanaugh moved to Pasadena to work for one year as a law clerk for Kozinski. And he continued to consult with Kozinski over the years.
Kavanaugh said he had never heard of Kozinski harassing laws clerks or engaging in improper behavior until it was revealed last year in news stories. “It was a gut punch for me,” he said.
Sen. Mazie Hirono (D-Hawaii) said she was skeptical of his response. “It was an open secret, and it went on for 30 years,” she said.
Sen. Cory Booker (D-N.J.) had a combative exchange with Kavanaugh while trying to pin the nominee down about his views on affirmative action. Booker asked if Kavanaugh believed that having a diverse student body is a compelling government interest that would justify considering race in admissions. Kavanaugh would not comment on his views, instead focusing on the Supreme Court’s precedent on affirmative action.
“I know what the law is now,” Booker said. “I’m worried about what the law is going to be when you get on the court.”
WASHINGTON — Landmark legislation that would rewrite the tax code and levy steep cuts to programs providing healthcare and food stamps to the poor passed the House early Thursday, a development that was celebrated by President Trump despite the bill facing an uncertain future among Senate Republicans.
The measure, titled the “One Big Beautiful Bill Act,” would boost funding for border security and the Defense Department, eliminate taxes on tips and overtime, provide a new tax deduction to seniors and renew the 2017 tax cuts passed during the first Trump administration. To pay for those new funding commitments, the bill proposes eliminating green energy tax benefits passed under President Biden, as well as an estimated $1 trillion in cuts to Medicaid and the Supplemental Nutrition Assistance Program.
Even still, the bill would add so much money to the debt that Congress may be forced to execute cuts across the board, including hundreds of billions to Medicare, in a process known as sequestration, according to the nonpartisan Congressional Budget Office.
The House vote fell along party lines. By opposing the bill, the Trump administration said that Democrats were supporting the largest tax increase on middle-class Americans in decades, a reference to the upcoming expiration of Trump’s 2017 tax cuts at the end of the year.
Democrats, on the other hand, have accused Republicans of voting for the deepest cuts to healthcare in modern times. By creating new barriers to Medicaid coverage through the introduction of work hour requirements, as well as increasing premiums under the Affordable Care Act, the CBO and other nonpartisan organizations estimate up to 14 million Americans could lose their insurance coverage.
Those drastic changes to the healthcare landscape have given pause to several Republican senators.
Sen. Susan Collins of Maine has said she is “very wary of cutting Medicaid.” Sen. Josh Hawley of Missouri said he “can’t support” substantial cuts to Medicaid benefits. And after the vote on Thursday, Sen. Roger Marshall of Kansas said that material changes should be expected to the House bill.
“We need to go back through that bill with a fine tooth comb and make it better,” Marshall said in an interview with Newsmax. “I think there’s opportunities in Medicaid to make that bill better, to make sure that we strengthen it, that we preserve it for those who need it most.”
Any Senate rollback of cuts to the Medicaid program could face resistance from the House Freedom Caucus during the reconciliation process. Members of that group, which proclaims a commitment to fiscal conservatism, have called for even deeper cuts to the Medicaid program.
Rep. Andy Harris of Maryland, chair of the House Freedom Caucus, voted “present” early Thursday morning, preserving negotiating leverage as the bill makes its way across Capitol Hill.
“I voted to move the bill along in the process for the president,” Harris wrote on social media. “There is still a lot of work to be done in deficit reduction and ending waste, fraud, and abuse in the Medicaid program.”
The vote came hours after Trump met with GOP holdouts at the White House. As late as Wednesday afternoon, before meeting with the president, several of those lawmakers were casting doubt on the prospects of the bill’s passage this week, ahead of a Memorial Day deadline set by House Speaker Mike Johnson, a Louisiana Republican.
Republican Sen. Lindsey Graham of South Carolina was dismissive of the Freedom Caucus on Thursday, telling CNN that the cuts they are pushing for would barely make a dent in the national debt.
“You had your chance,” Graham said to the caucus. “Some of these cuts are not real. We’re talking about over a decade — you know, if you do $1.5 trillion, that’s like a percent and a half. So let’s don’t get high on our horse here that we’ve somehow made some major advancement of reducing spending, because we didn’t.”
Sen. Kevin Cramer of North Dakota also mocked the caucus, calling it “rich” for its members to lecture Senate Republicans on fiscal conservatism, “and end up with not that conservative a bill.” The CBO estimates the House legislation would result in a $3.8-trillion increase to the deficit.
If passed, the new work requirements to Medicaid would kick in at the end of 2026, right after the midterm elections. Green energy tax credits would phase out for any project that is not already under construction 60 days after the law comes into force.
The cap on the state and local tax deduction, known as SALT, will increase to $40,000 from $10,000, phasing out for individuals and households making more than $500,000. And while the president campaigned on a promise to eliminate taxes on Social Security, a parliamentary rule precluded Republicans from including a full cut. Instead, the bill proposes an enhanced tax deduction for senior citizens of up to $4,000.
On Truth Social, the president’s social media platform, Trump wrote that the bill is “arguably the most significant piece of Legislation that will ever be signed in the History of our Country!”
“There is no time to waste,” he added. Johnson, the speaker, has set a goal of sending the bill to the president’s desk by Independence Day.
Trump’s press secretary, Karoline Leavitt, said the president’s team was “suiting up” for negotiations with the Senate now that the bill has passed the House. “We will see how it goes,” she said.
“The ‘One Big Beautiful Bill’ is named the ‘One Big Beautiful Bill’ for a reason, because it is a one big beautiful bill that encompasses just about everything this president could want for the American public. It delivers on so many of his core campaign promises. So surely we want to see those campaign promises signed into law,” Leavitt said. “He’s expecting them to get busy on this bill and send it to his desk as soon as possible.”
The two House Republicans who voted against the bill, Thomas Massie of Kentucky and Warren Davidson of Ohio, should face primary challenges for their defiance of the president’s directive, Leavitt added.
“What’s the alternative, I would ask those members of Congress. Did they want to see a tax hike? Did they want to see our country go bankrupt? That’s the alternative by them trying to vote no,” she said. “The president believes that the Republican Party needs to be unified.”