Trump says we need a government shutdown. Here’s what’s happened in the past
It’s a political gambit that
“Our country needs a good ‘shutdown’ in September to fix mess,” he tweeted last week.
The unconventional proclamation from the unconventional president raised concern from both sides of the aisle.
His comments came as lawmakers agreed to a $1-trillion bipartisan budget bill that funds the federal government through September, which means another battle and potential government shutdown looms this fall.
Under a shutdown, thousands of federal employees would go without pay and national parks would close, among other things. In short: It will upset a lot of people.
Here’s a look at the key players and fallout from recent government shutdowns.
October 2013
How it happened
It’s simple — the battle over healthcare closed the government.
That year, House Republicans, angered by
The government shut down for more than two weeks after
On the political front, the ramifications went both ways.

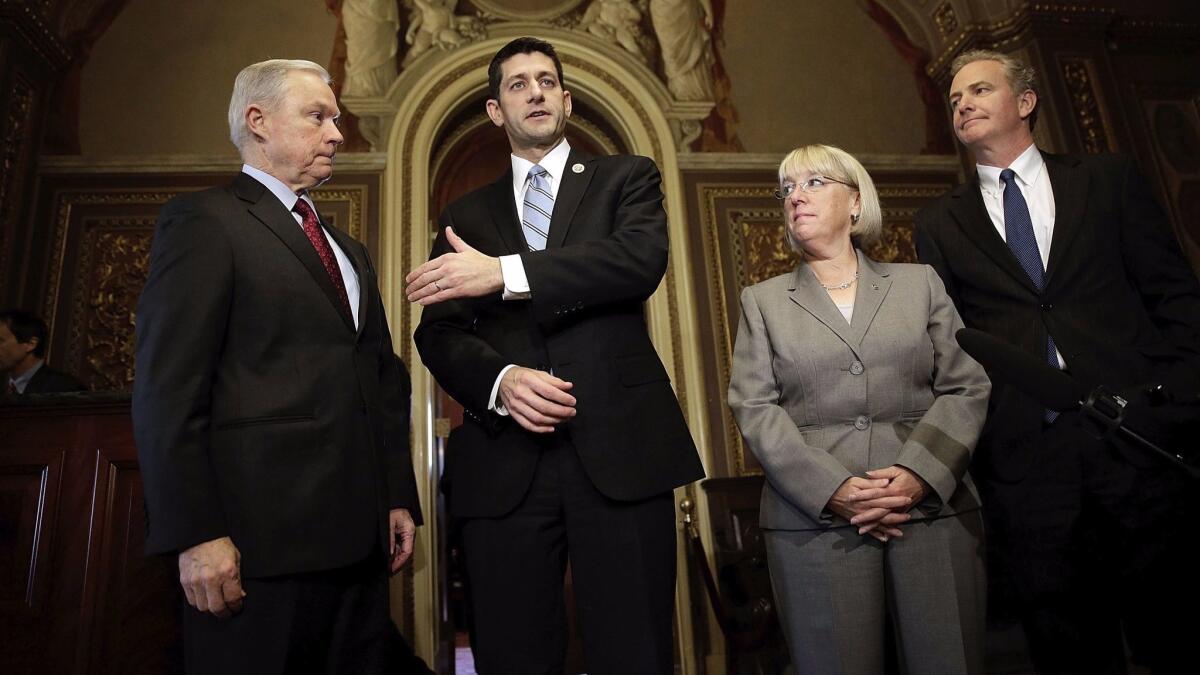
Members of the bipartisan budget conference Sen. Jeff Sessions (R-Ala.), Rep.
(Win McNamee / Getty Images)
Winners
Sen. Harry Reid (D-Nev.)

(Alex Wong / Getty Images)
The then-Senate majority leader was a vocal Democratic critic of Republican-led efforts to defund President Obama’s healthcare bill. He relentlessly castigated Republicans for their tactics to defund Obamacare, which ultimately led to the shutdown.
“You know with a bully you cannot let them slap you around, because they slap you around today, they slap you five or six times tomorrow. We are not going to be bullied,” Reid told reporters.
In the end, Reid came out of the shutdown with a bolstered reputation as a fighter of Democratic causes and earned plaudits from Obama.
Obamacare

(Gary Friedman/Los Angeles Times)
At the time, the botched rollout of the healthcare law drew daily headlines. Web sites for healthcare exchanges didn’t work and the administration had few answers. Still, the healthcare law was able to remain intact and public scorn focused on Republicans as the government remained shuttered for 16 days and federal employees nationwide stayed home. Republicans thought their efforts would prove fruitful.
Sen. John McCain (R-Ariz.)

(T.J. Kirkpatrick / Getty Images)
In the months and weeks leading to the shutdown, McCain served as a voice of reason for the Republicans. He insisted that it would be unwise for the party to allow a shutdown over Obamacare.
“I campaigned in 2012 all over this country for months: ‘Repeal and replace Obamacare.’ That was not the mandate of the voters. If they wanted to repeal Obamacare, the 2012 election would have been probably significantly different,” he said at the time.
Ultimately, his efforts faltered as Republicans charged ahead with efforts to defund Obamacare and the government shutdown.
Losers
House Speaker John A. Boehner (R-Ohio)

(Alex Wong / Getty Images)
He failed to rein in the most conservative grassroots wing of his party. Boehner was the middle man of sorts in negotiations between Democrats, moderate Republicans and conservative activists. Two years later, he resigned because of the strong opposition he faced from the Republican caucus.
Sen. Ted Cruz (R-Texas)

(Andrew Burton / Getty Images)
While Cruz raised his national profile as a staunch critic of Obamacare, he also made a lot of enemies. Weeks before the shutdown he delivered a 21-hour talkathon on the Senate floor, assailing the health care law — a move that drew scorn from Democrats and Republicans alike. Cruz’s vocal opposition to the law helped establish him as a force within the GOP grassroots and set him up for a presidential run in 2016.
Debbie Wasserman Schultz (D-Fla.)

(Carolyn Kaster / Associated Press)
(Carolyn Kaster / AP)
Public opinion polls consistently showed that Republicans were blamed for the government shutdown. Even so, the former Democratic National Committee chairwoman was unable to turn that into victory in the 2014 midterm. Many Democrats fault her leadership as a factor in the party’s sweeping losses in the midterm election.
November/ December 1995 and January 1996
How it happened
This battle over funding

President Clinton and bipartisan leaders meet at the White House on Dec. 30, 1995, for talks on the federal budget. (Greg Gibson / Associated Press)
(GREG GIBSON / AP)
Winner
President Clinton

(Marcy Nighswander / Associated Press)
(Marcy Nighswander / AP)
He stood firm in his battle with the Republican-controlled Congress. Clinton wanted a budget that increased expenditures on, among other things, Medicare and public education, but Republicans wanted to slow government spending. This led to months of negotiations — the government closing, opening, then closing again — and through it all, Clinton’s public approval ratings dipped only slightly. He easily won reelection in November 1996.
Loser
House Speaker Newt Gingrich (R-Ga.)

(J. Scott Applewhite / Associated Press)
(J.SCOTT APPLEWHITE / AP)
After sweeping gains in the 1994 midterm election, Republicans were emboldened and ready for a showdown.
“He can run the parts of the government that are left, or he can run no government,” Gingrich told reporters weeks before the first shutdown. “Which of the two of us do you think worries more about the government not showing up?”
News reports at the time also noted that Gingrich was open to a shutdown after Clinton made him exit the rear of Air Force One after the two attended the funeral of slain Israeli leader Yitzhak Rabin. The comments made the Republican leader appear petty. In the end, after weeks of a shutdown, Republicans ultimately conceded to Clinton and Democrats.
May 2017
What’s happening now
Last week Congress passed a $1-trillion budget that funds the federal government through September. However, the budget bill does not allocate funds for Trump’s much-promised border wall. It’s the first bipartisan piece of legislation of the Trump presidency and funding for his signature proposal is nowhere to be found. The bill, however, does have funding for border security and increases to defense spending — both of which were touted as wins by the Trump administration.

Senate Majority Leader Mitch McConnell (R-Ky.), flanked by Sen.
(Aaron P. Bernstein / Getty Images)
Key players
President Trump
It’s clear Trump does not like to lose and does not like bad headlines. By all accounts, Trump and his policies did not come out on top in the budget deal.
Trump blamed the Senate rules, which require 60 votes to pass most legislation, for the exclusion of key priorities from the spending bill.
This has in turn led some conservatives to push for Trump to support a government shutdown if Congress does not heed his policies this fall. Trump has always trusted his gut instinct in politics — so far it’s seemed to benefit him — and his comments will be closely watched this fall.
House Speaker Paul D. Ryan (R-Wis.)

(J. Scott Applewhite / Associated Press)
He’s often had to stake out a position when Trump tweets. Indeed, this time was no different. Ryan alluded to Trump’s qualms with Senate rules.
“Look, we’ve got a long ways to go between now and September, but I share the president’s frustration,” Ryan told reporters. “What a lot of people in America don’t realize is appropriations bills, they take 60 votes to pass. They can be filibustered. So, all appropriations bills therefore have to be bipartisan because Democrats can always filibuster an appropriations bill. Having said all that, I feel very good about the wins that we got with the administration in this bill.”
Senate Minority Leader Charles E. Schumer (D-N.Y.)

(J. Scott Applewhite / Associated Press)
He’s Trump’s chief critic in Congress and warned the president that a government shutdown is not wise.
“The president’s threat to shut down the government in September is just a very, very bad idea because it would hurt so many average folks,” Schumer said recently. “I strongly urge my colleagues, and they have already … said they have no desire to shut down the government. That is not the way to govern. That is not the way to come up with bipartisan compromise.”
Voters
Public opinion is not on Trump’s side when it comes to talk about a government shutdown.
In a Politico/Morning Consult poll released in April, 65% of voters said that Congress should “take all necessary steps to avoid a government shutdown.”
Other polls show similar disapproval among voters toward a government shutdown.
Twitter: @kurtisalee