101 East meets the doctors using drones to fight tuberculosis and save lives in remote communities in the Philippines.
Tuberculosis is a leading cause of death in the Philippines, killing an estimated 98 people each day.
The infectious disease is particularly grave in remote communities, where medical services are limited and delayed diagnosis and treatment can be fatal.
But a Filipino doctor is determined to change that with modern innovations.
Dr Heidi Sampang uses drones to fly samples and speed up testing.
The technology can help save lives by expediting the delivery of essential medical supplies in a country with thousands of mountainous islands.
101 East meets the medical teams using drones to fight tuberculosis in the Philippines.
Tokyo, Japan – While walking his toy poodle in the park near his home in Ikeda, Gifu Prefecture, Shin Ohta had an idea.
“My dog often stops walking during our strolls. I would carry him every time, but his weight of nearly 5kg [11lbs] started to become a real burden,” Ohta told Al Jazeera.
Recommended Stories
list of 4 itemsend of list
“I knew there had to be a better way.
Ohta works in sales for Japan’s oldest baby carrier manufacturer, Lucky Industries, which has produced more than 40 million baby carriers since its founding in 1934.
He has spent his career making baby carriers, but after that walk, he wondered if the same expertise could be applied to pets.
After consulting a veterinarian to ensure the design was viable for dogs, Ohta helped Lucky Industries launch its first line of dog hip carriers in 2022: Nu-i.
Earlier this year, the company joined dozens of other brands at Tokyo’s annual Interpets conference, a showcase of Japan’s rapidly growing pet care market.
During the first weekend of April, stalls lined the walls of the Big Sight convention centre, selling everything from walk-in pet dryers to the latest organic cat treats.
Few of the pet owners attending the event had their four-legged friend on a leash, instead ferrying them to and fro in well-decorated pet strollers, or the doggy equivalent of baby slings.
Many pets were decked out in colourful outfits, fur clips, and diapers.
Pets in Japan now outnumber children under 15 by more than 2 million.
Unicharm displays products at the Interpets Conference, held at the Tokyo Big Sight Conference Centre in Tokyo, Japan, on April 3, 2026 [Genevieve Mansfield/Al Jazeera]
According to market intelligence company Euromonitor, the country’s pet care market was worth 880 billion yen ($5.4bn) in 2025, up from 689.6 billion yen ($4.2bn) in 2020.
As Japan’s birthrate continues to fall and the population of children shrinks, companies that once built their businesses on babies, selling nappies, slings, and strollers, are increasingly turning their attention to pets.
Betting on pets at the Interpets conference, Unicharm’s expansive stall was lined with dog and cat nappies from its latest “Mannerware’” line.
The Tokyo-based company has been one of the great cross-market successes of the pet care boom.
After making its name selling feminine hygiene products and disposable diapers, Unicharm expanded into pet diapers in 2001.
Since then, pet care products have become one of the company’s main growth engines.
While the personal care market for people is larger, the pet care sector has higher profit margins.
According to Unicharm’s financial results for 2025, the company’s pet care division had a profit margin of 15.4 percent that year, compared with personal care’s margin of 10.7 percent.
Isshu Uehara, a Unicharm spokesperson, said that as of 2025, the pet care business accounted for 17 percent of the company’s total sales, with plans to increase that share to 20 percent by 2030.
“Japan’s birthrate is declining,” Uehara told Al Jazeera.
“Lifestyle changes, such as remaining single, marrying late, and the growth of childless, dual-income households, have led to a greater number of people seeking emotional connections through pets.
“As a result, we’re seeing the growth of ‘pet humanisation’, or treating pets like family members or children rather than just animals.
“Customers want to buy premium products to extend pets’ lifetimes, and share experiences with them, like dining together or going out to cafes and friends’ houses,” Uehara added.
Two pets pose at the Interpets Conference on April 5, 2026 [Genevieve Mansfield/Al Jazeera]
Unicharm is not alone.
Across Japan, stroller brands like AirBuggy and clothing companies like Sweet Mommy have made similar leaps, applying expertise built around infants to a growing market of pet owners.
Lucky Industries CEO Hiroyuki Higuchi pointed to the company’s origins to explain the shift towards pets.
“When the company started, Japanese families had many children, and mothers needed carriers to be able to work around the house,” Higuchi told Al Jazeera.
But now, Japanese families are shrinking. While there has been a rise in single-person households and childless dual-income households, families with only one child have become more common as well.
A national survey of fertility trends found that between 2002 and 2021, the proportion of households with only one child increased from 10 percent to nearly 20 percent.
“With fewer babies around, it has been harder to come up with new ideas for baby products,” Ohta said.
“Now, my life is centred around my dogs, as are the lives of many of my friends. When we meet up, we talk about our pets.”
“Compared to the baby goods market, the pet sector is doing better,” said Higuchi.
“Companies see it as a reliable sector… In Japan, dogs are seen as babies, as part of the family. Just like many Japanese carry their babies in slings or carriers, so can dog owners,” Higuchi added.
Unicharm displays pet care products at the Interpets Conference on April 3, 2026 [Genevieve Mansfield/Al Jazeera]
Barbara Holthus, a sociologist and director of the German Institute of Japan Studies, said pet humanisation has been a growing trend in recent years.
“Before, a dog or cat might have just been an additional family member, but with fewer other family members and fewer children in the house, the focus becomes very concentrated on this animal,” Holthus told Al Jazeera.
“But it’s more diverse than just replacing children. Animals take on many different roles,” Holthus added. “A pet can also replace a partner. After a divorce, people sometimes get pets.
After someone gets widowed, they get a pet. Sometimes, a pet is seen as a play partner for an only child.”
Holthus sees Japan as a prime example of changing family structures, including the emergence of the “multi-species family”.
Holthus said decreasing birth rates, as well as factors such as loneliness and rising urbanisation, help explain why the trend of humanising pets has been particularly pronounced in Japan.
As for why infant brands are turning to pets, Holthus offered a simple explanation.
“It’s understandable,” she said.
“Of course, companies want to make money, and due to demographic change, their market is getting lost.”
CONCORD, N.H. — Two transgender girls who were the first to challenge President Trump’s executive order, “Keeping Men Out of Women’s Sports,” have withdrawn their lawsuit in New Hampshire based on a recent U.S. Supreme Court ruling that upheld state bans on transgender athletes in girls’ sports and their own personal hardships, their lawyer said.
“This case was always about two courageous young girls who simply wanted the same opportunities as their peers to participate in school life,” their lawyer, Chris Erchull of GLAD Law, said in a statement Thursday. “Their willingness to stand up to extraordinary hostility made clear the human cost of laws that target transgender youth.”
The teenagers, Parker Tirrell and Iris Turmelle, took on Trump’s executive order last year, amending their 2024 complaint against New Hampshire’s law on banning transgender girls from school sports. A federal judge had granted a court order allowing them to play as the case proceeded.
For Tirrell, it meant being able to keep playing on her high school girls’ soccer team. For Turmelle, it was having a chance to try out for different sports.
Both sides agreed to pause the case and wait for a ruling from the Supreme Court as it considered similar state laws barring transgender girls and women from playing on school and college athletic teams in Idaho and West Virginia. Last month, the court upheld the laws. It also said that barring transgender girls and women doesn’t run afoul of the federal law known as Title IX, which prohibits sex discrimination in education.
One teen and her family decided to move from New Hampshire
Turmelle and her family moved out of New Hampshire last summer following proposed legislation against transgender people. One measure signed into law by Republican Gov. Kelly Ayotte last year prohibits medical professionals from providing puberty blockers and hormone replacement therapy to new transgender patients under age 18.
“Though there may be a carve-out for people already receiving gender-affirming care, that is way too close a call for us to risk staying,” Turmelle’s mother, Amy Manzetti, wrote in an op-ed piece at the time. “Other New Hampshire laws also seek to erase her.”
Most Republican-controlled states in the past five years have adopted laws or policies limiting gender-affirming care for transgender minors and limiting which school bathrooms transgender people can use, as well as sports restrictions. The Williams Institute at UCLA estimates that about 3% of youth ages 13 to 17 identify as transgender.
“The challenges with relocation are significant and burdensome — this includes having to find new employment, buying and selling homes, packing and moving possessions, integrating kids with a new school system, losing access to longstanding family and friends, and potential loss of income,” Corinne Goodwin, the executive director of Eastern PA Trans Equality Project in Pennsylvania, said in an email.
“But these families do so because they love their kids and know that supporting them with the care and opportunities they need is critical to their long-term success and happiness.”
The other teen gave up playing soccer at high school
Tirrell, 17, began her junior year last fall on the girls’ junior varsity soccer team. Things were fine at first, and each time she scored a goal, she got a round of ice cream from her parents. But a few weeks into the season, she decided to stop playing.
“With all of the political stuff going on, soccer wasn’t just about the game anymore,” her mother, Sara Tirrell, told The Associated Press in an interview.
It became more about preparing for the possibility of conflict.
“Were there any local Facebook groups where they were sort of agitating about potential protests and how do we prepare, and what are we walking into, and we never kind of knew,” she said. “We were on a lot of pins and needles, especially after the previous season.”
She was referring to a controversy at an away game where two dads from an opposing team were banned from school grounds for wearing pink wristbands marked “XX” to represent female chromosomes. They sued the school district and a judge ruled against them. They have appealed their case.
Last fall, there was an increased presence of school administrators at the games and bus drivers pulled in closer to the field so the students weren’t in the parking lot, she said.
“Parker didn’t talk about it a lot, but I think she could see that stress for everybody — for her, for her teammates, for her coaches,” Sara Tirrell said. “She felt kind of bad about pulling them all into that circus again. And so she ultimately said, ‘This isn’t fun anymore and I don’t want to do it.’”
Parker’s father described the atmosphere as “palpable tension.”
Even playing on her own turf, “there would typically be a couple of police officers at the home games where there weren’t previously,” Zach Tirrell said.
In the past, Parker also played soccer in a recreation league and could still do so.
“But I think it all kind of still sort of weighs on her,” her mother said. “It’s the same group of kids that she plays with who, honestly, have been very supportive and love to have her on the team and have expressed that to her many times over. But I think she still has that worry in her brain around, ‘What are other people going to say and do if I show up at a game?’”
Parker’s parents hope she’ll return to playing soccer some day. In the meantime, “she plans to be around and use her voice to continue standing up to discrimination,” her mother said. “In some ways she’s had to grow up a lot faster than some of her peers.”
McCormack writes for the Associated Press. AP writer Geoff Mulvihill in Haddonfield, N.J., contributed to this report.
Checking a little-known page could help you find cheap flights, even in the six-week school holidays, and if you’re not fussy about your destination you can save on a family getaway
This article contains affiliate links, we will receive a commission on any sales we generate from it. Learn more
The page includes deals on school holiday dates(Image: Getty Images)
The school summer holidays are in full swing in Scotland, and looming for parents across England and Wales, meaning there are going to be families up and down the land looking for inexpensive ways to get away.
Unfortunately, going away with the kids during the six-week break is never going to be an inexpensive undertaking, but if you aren’t fussy about the destination and just want some sunshine, a little-known webpage could be a good place to start.
Simply enter the dates you’d like to depart, plus airports you want to fly from, and you’ll find a list of the cheapest places to take the family. The more flexible you can be, the better the deals, so midweek departures and choosing a slightly farther airport could help cut your costs.
TUI airways’ dedicated Cheap Flights page is where you’ll find inexpensive return tickets for selected routes for unbooked or returned seats. The best deals are often found on last-minute dates, as the airline looks to fill remaining capacity.
Best of all, unlike many cheap flight deals, flying with TUI Airways on a flight-only ticket gives you two pieces of hand luggage per adult and child. You can take one small personal item like a handbag or laptop bag that’s small enough to fit under the seat in front of you, with maximum dimensions 40x30x20cm, as well as a 10kg bag per passenger of maximum dimensions 55x40x20cm.
Checked-in bags and seat selection cost extra, but TUI says: “If you’re flying with TUI Airways and there’s a child under the age of 12 on your booking, we’ll make sure they’re seated with at least one adult in your party.”
It’s worth noting that this can mean they end up sitting in front of you or across an aisle, so consider whether you want to pay to select your seat.
TUI’s flights operate from more than 20 UK airports and cover over 100 destinations, so you may find a hidden gem using this tool that you might have otherwise missed. Return flights on this tool can start at as little as £30 return, and you’ll find both short-haul destinations such as Spain, Greece, and Italy, as well as long-haul routes from the Caribbean to Mexico and Thailand.
Cheap deals in the next couple of weeks from Scotland include a £70 fare from Glasgow to Reus, departing July 11 and returning July 25. While parents in England and Wales can choose from school holiday deals such as a £70 return from Bournemouth to Ibiza from July 18 to 29, just at the start of the six-week break, or London Gatwick to Split, Croatia for £128 return from July 20 to 27. However, seats for these deals are extremely limited and will sell out very quickly.
Flight search aggregator sites such as Skyscanner are also a great way to find the best deals. Simply choose ‘everywhere’ as your destination and tick ‘add nearby airports’ if you’re willing to fly from a different hub.
A family travel advisor at Lapland Famille, who plans full Arctic adventures, advised parents to consider the total cost of the journey, not just the headline fare. “A very low flight price can be a brilliant find, but families need to look at the whole trip before booking.
“If the cheapest option means difficult flight times, separate seats, extra baggage costs or a long transfer with tired children, the saving can disappear quickly. The best-value holiday is usually the one where the total cost, timing and stress level all work for the family.”
Have a story you want to share? Email us at webtravel@reachplc.com
WASHINGTON — A Democratic U.S. senator warns the Trump administration is getting ready to round up 500 immigrant children in a hasty effort to remove them from the country, bypassing legal protections. It would be their second attempt after a federal court intervened last year in an overnight plan to fly out hundreds of children on Labor Day weekend.
Sen. Ron Wyden of Oregon wrote in a letter Wednesday to U.S. Health Secretary Robert F. Kennedy Jr., which oversees the Office of Refugee Resettlement caring for unaccompanied migrant children, that he had “credible information” that the Trump administration had a list of more than 500 migrant children it was targeting for a fast-track removal process and that the department was racing to act in days. He warned that the administration was abdicating “core humanitarian and child welfare mandates” and demanded an immediate halt to any plans to remove the children.
Wyden, who is the ranking member and senior Democrat of the Senate Finance Committee, which has jurisdiction over ORR, did not detail how he came by his information. His office declined to provide further details. ORR falls under the Department of Health and Human Services.
An HHS spokesperson denied any such plans.
“The new information I obtained leads me to believe that the Department is laying the groundwork for another lawless deportation effort, this time on a greater scale, across more countries of origin,” Wyden wrote.
“You have been entrusted with the care and safety of the children placed within the ORR network. Proceeding with this plan knowingly endangers their lives and violates your duty to these vulnerable children.”
Wyden also issued an early warning last August ahead of what eventually became a chaotic weekend of efforts by the Trump administration to remove Guatemalan children in its care and send them home.
HHS spokesperson Emily Hilliard said in “there are no plans to target these children,” calling Wyden’s claims ”irresponsible fearmongering.”
“The Trump Administration is working to identify the parents or legal guardians of unaccompanied alien children in our care because ensuring every child is placed with a properly vetted sponsor is our top priority,” she said.
Over the Labor Day weekend, dozens of migrant children either staying in government-supervised shelters or with foster families were taken from their homes and bused to airfields in Texas bound for Guatemala. A federal judge woken up in the middle of the night eventually stopped the planes. Lawyers for the children — many who had fled violence at home to come to the U.S. — later described how traumatic the middle-of-the-night removal effort was for them.
The administration insisted it was reuniting the Guatemalan children — at the Central American nation’s request — with parents or guardians who sought their return. Lawyers for at least some of the children said that wasn’t true and argued that in any event, authorities still would have to follow a legal process that they did not.
Migrant children traveling alone are usually entrusted to U.S. government care, and there are various legal protections designed to protect them once they’re in the U.S. and navigating the immigration system.
The Trafficking Victims Protection Reauthorization Act of 2008 is one of the key pieces of legislation designed to protect them. With some limited exceptions, it requires that children be placed in the “least restrictive setting possible,” which generally means that they can be released to a sponsor such as a relative in the U.S. while their immigration proceedings play out.
The children can apply for a specially protected status if they can’t return to their home country because of abuse or neglect and they can also apply for asylum.
The Trump administration has made it increasingly difficult for those children to be released to sponsors though. The administration says that they are doing due diligence to make sure that sponsors are thoroughly vetted and that in the past, children were released into dangerous situations.
But advocates say that the result has been children lingering for months in government shelters.
This time, Wyden said the children at risk of being removed come from various countries, potentially including Guatemala, Honduras, El Salvador, and Afghanistan, and have been in U.S. custody — mainly in foster care — for at least 180 days. He said they were described as not having any “viable sponsor” who could come forward and take care of them in the U.S.
Not having an identified sponsor could mean the child’s parents are in their home countries, are deceased or are too afraid to claim their children after ICE started arresting some parents who are not in the country legally during their reunification efforts.
Gonzalez and Santana write for the Associated Press.
In Lincoln Park, past Plaza de la Raza cultural center and under swaying pine trees, stands a row of 10-foot wooden panels etched with names. Robert Zaldivar stood quietly in front of the names, surrounded by community members holding lit candles as memories of old friends resurfaced.
The panels bear nearly 2,000 names, and more are added every year. Each one represents an Angeleno, mostly Latinos, who died of AIDS. Zaldivar led the movement to erect this monument, named the Wall Las Memorias, which was finalized in 2004.
Inspired by his late best friend, who was HIV-positive, the Wall represents to Zaldivar the power of remembering those in his community affected by HIV and AIDS. It was designed in the shape of Quetzalcoatl, or the “Feathered Serpent,” an Aztec deity and symbol of rebirth.
Robert Zaldivar leads a sunset vigil at the Wall Las Memorias AIDS Monument in Lincoln Park on the anniversary of the first HIV diagnosis in L.A. on June 4, 2026.
(The Wall Las Memorias)
That day in early June, he hosted a sunset vigil, joined by AIDS Memorial Quilt founder and Harvey Milk mentee Cleve Jones, to recognize the lives lost since AIDS was first diagnosed 45 years prior, when the Centers for Disease Control and Prevention published a report detailing immunodeficiency in five young gay men in Los Angeles.
At Zaldivar’s feet was a poem, one he wrote in 1995 with his friend Anna Contreras.
It reads:
It is here, we free ourselves from the teaching of guilt. We unite as one people in our vision, our teaching, and our truth. Through truth we live, through knowledge we survive.
Contending with stigma and misinformation has been a constant struggle for people who are HIV-positive, he said, a struggle that Zaldivar hopes to make more visible now than it has been in previous decades.
“Sometimes it feels like there’s no other way to draw attention to this problem than to have a physical reminder,” Zaldivar said of the monument. “This reminds us of real people, as more than statistics.”
The statistics Zaldivar refers to include the continuing rise in HIV diagnoses in Latinos across the United States. The most recent CDC data show 39,000 people across the U.S. received an HIV diagnosis. And a Kaiser Family Foundation analysis revealed that between 2010 and 2022, there was a 24% increase in new cases among Latinos. In 2022 alone, Latinos made up 31% of new diagnoses, despite only representing 19% of the American population, the KFF study found.
“Just last week, we had two new diagnoses of HIV in our clinic,” said Bernardo Gomez, assistant manager of HIV resources at the Wall Las Memorias Project. “For context, we had 15 in the past six months, including straight women … I think what we’re seeing is a dangerous loss of support for outreach and education.”
Last year, President Trump released his presidential fiscal year budget for 2026, much of which went into effect last October. In it, he revealed significant cuts to HIV health programs — amounting to $1.5 billion.
The budget recommendation signaled the administration’s yearly priorities, and Trump’s fiscal plan and staffing cuts to HIV teams under the so-called Department of Government Efficiency (DOGE) showed a shift away from HIV prevention and healthcare, which advocates say has led to providers losing jobs and places for testing and resources to shrink. In L.A., the Latino community is feeling the brunt of the loss, Zaldivar said.
The biggest cut to HIV care in the 2026 budget affected the CDC, which lost around $3.6 million. Another devastating loss was $1.7 million cut from the Ryan White HIV/AIDS Program, which many L.A. resource centers report relying on to fund part of their programming and staffing.
Robert Gamboa, associate director of public policy at the L.A. LGBT Center, said that in Trump’s first term, his “Ending the Epidemic” program created hope for soon seeing the end of HIV in the U.S. — a hopefulness that he said was quickly dashed in his second term.
“Now there’s this 180-degree shift in policy, we see these enormous proposals pulling away from funding, and his lack of acknowledgment of World AIDS Day, and Pride in general,” Gamboa said. “The message of that is loud and clear: [The Trump administration] is telling our LGBT community, ‘We don’t care about you.’”
Since Trump’s inaugural address last year, Gamboa said executive orders have only solidified Trump’s shift away from LGBT organizations, “challenging the structural integrity of almost everything we’ve done.”
Gamboa said that last spring, the Department of Public Health, Division of HIV and STD Programs), which supplemented L.A. organizations with substantial HIV funding, sent out a notice that all of their contracts were terminated.
“Well, this caused a massive alarm all across L.A. County. Everyone started freaking out. We had to say, ‘We need an emergency allocation [from state funds] so that we can continue providing HIV services across California,’” Gamboa said. “We’re used to getting upwards of around $20 million in funding at the county level, and it wasn’t happening.”
Robert Zaldivar leads a sunset vigil at the Wall Las Memorias AIDS Monument in Lincoln Park on the anniversary of the first HIV diagnosis in L.A on June 4, 2026.
(The Wall Las Memorias)
Since then, nonprofit representatives have confirmed that the contracts were restored at reduced rates. However, the impact of the uncertainty shook the health services community and only caused further distrust among Latino patients.
“We’re already seeing [the impact in L.A.]. In the Latino community, there’s so much fear from the ICE raids. People are afraid to even leave their homes,” Gamboa said. “We’ve worked so hard in building trust and relationships with our communities of color. Now, they’re afraid to even come in. Many of the places they’ve gone to in L.A. County have already closed their doors and ceased services.”
Most recently, the Trump administration announced plans to cut millions in public health funding. This includes $1.1 million that would be slashed from the National HIV Behavioral Surveillance Project, an early-warning system for HIV outbreaks, established by the L.A. County Department of Public Health.
On the White House website, a page called “Cuts to Woke Programs” reads: “President Trump is committed to eliminating radical gender and racial ideologies that poison the minds of Americans.”
Gamboa said that organizations have been discouraged of using “LGBT” in their programming to avoid being defunded as part of the targeted “woke” programs.
“It really affects me,” said Gomez, who has been living with HIV since 1996. “How long will I have medicine?”
Gomez, who is the breadwinner of his family, says his monthly supply of medication costs $1,500 a bottle. “It’s so expensive, and I have insurance. For people without insurance, [the Ryan White program] is the only way they can afford treatment,” Gomez said. “I’m afraid of what will happen to them.”
Gomez takes antiretroviral therapy, a lifesaving medication that reduces the number of infected cells, making the disease less transmissible and prevents HIV from developing into AIDS. According to 2024 HRSA data, the Ryan White program provided antiretroviral therapy to 602,000 people, preventing the spread of HIV.
As the program loses funding, jobs providing HIV care have become more sparse — and programs like the Wall and the L.A. LGBT Center have become more essential to support the thousands left without life-saving care.
HIV program funds are trickling back into L.A. County for nonprofits this year; although some, like the Wall, maintain that it’s “not enough to address the need.” Up until last May, the organization shared that the county funded $1 million of its annual HIV reduction efforts. This year, that number was drastically reduced to $100,000 per six-month contract.
“Many of my social worker friends are off the streets [where they helped at-risk communities] due to just not having enough funding to do their jobs,” said Miguel Rodriguez, program coordinator of HIV testing and prevention at the Wall. “People think only gay men are affected, but basic sexual health for everyone is at risk here. Less [testing] means more infections and transmissions across the board.”
As Robert Zaldivar stresses, the only way to protect L.A.’s Latino HIV-positive community is to support remaining HIV services to get tested or donate to local service organizations.
“What we saw in the ’90s, I’m scared that it will repeat. I want people to remember how serious [HIV] is, and to educate,” Zaldivar said. “Keep getting tested. We don’t report your immigration status or sexuality. Just come in.”
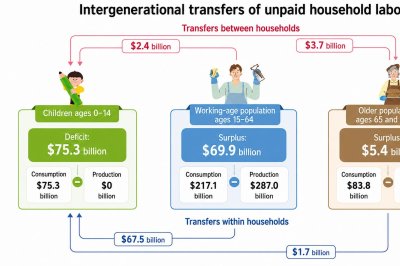
A chart illustrates how the estimated value of unpaid household labor is transferred among children, working-age adults and older people in South Korea. Information from Ministry of Data and Statistics. Infographic by Asia Today and translated by UPI
June 23 (Asia Today) — The estimated value of unpaid household services consumed by South Korean children totaled 116.6 trillion won ($75.3 billion) in 2024, with parents and grandparents providing much of the work, government data showed Tuesday.
The Ministry of Data and Statistics published the findings in South Korea’s 2024 National Time Transfer Accounts, which measure how unpaid household work is produced, consumed and transferred among age groups.
The account covers services that are generally excluded from gross domestic product, including cooking, cleaning, household management, caregiving and volunteer work.
The figure does not represent money that families paid for child care. It estimates the market value of unpaid services by using the time spent on household work, population figures and the wages that would be required to hire someone to perform similar tasks.
Children ages 14 and younger recorded a household-work lifecycle deficit of 116.6 trillion won because they consumed unpaid services but did not produce them.
A lifecycle deficit occurs when the value of household services consumed by an age group exceeds the value it produces.
About 107.3 trillion won ($69.3 billion), or 92% of the children’s deficit, was covered through transfers within the same household. This category largely represents time and labor provided by parents and other family members living with the children.
An additional 9.4 trillion won ($6.1 billion) came through transfers between households, which can include care provided by relatives living separately.
Working-age people between 15 and 64 produced unpaid household services valued at 444.4 trillion won ($287 billion) and consumed services worth 336.1 trillion won ($217 billion).
That left the group with a surplus of 108.3 trillion won ($69.9 billion).
The working-age population transferred a net 104.6 trillion won ($67.5 billion) in unpaid services to other members of the same households, primarily children.
The data show that people in their 30s and 40s, who are often raising young or school-age children, were at the center of the transfer system.
On a per-person basis, the household-work surplus reached its highest level at age 39, at 10.35 million won ($6,700).
Older South Koreans also made a net contribution.
People ages 65 and older produced household services valued at 138 trillion won ($89.1 billion) while consuming 129.7 trillion won ($83.8 billion), leaving a surplus of 8.3 trillion won ($5.4 billion).
They transferred a net 5.7 trillion won ($3.7 billion) in services between households. The ministry said the pattern reflects contributions such as grandparents caring for grandchildren who live in separate households.
Per-person household production peaked at age 40, declined and then increased again after retirement, producing what the ministry described as an M-shaped pattern.
Unpaid housework and care for grandchildren contributed to the later increase.
The lifecycle deficit was highest at birth, reaching 37 million won ($23,900) per person.
The balance shifted into a surplus at age 28, reached its peak at age 39 and returned to a deficit at age 82.
Those ages do not indicate when income begins to exceed personal spending. They show when the estimated value of unpaid household services a person produces becomes greater or smaller than the value of services the person consumes.
Household-service consumption was highest at birth and lowest at age 19, forming an L-shaped pattern.
Compared with 2019, the total deficit for children declined by 7.5 trillion won ($4.8 billion). Surpluses among working-age and older people also decreased.
The results provide a broader measure of the economic contributions made inside families, including work performed by parents and grandparents that does not appear in conventional income or production statistics.
THE Traitors star Diane Carson has revealed she suffered a nasty fall on holiday that resulted in a £280 trip to the dentist.
The keen runner, 65, is on holiday in Lisbon with her son and his girlfriend, Rima.
Sign up for the Showbiz newsletter
Thank you!
The Traitors star Diane Carson injured her tooth in a jogging accidentCredit: Instagram/dianeakamumDiane is one of the best-loved Traitors starsCredit: BBC
While exploring the sunny Portuguese city, Diane came a cropper on a jog and it needed a pricey resolution.
She shared a video of her happily bounding through a park before the accident and wrote over the top: “Today’s amazing run — before the £280 worth of dental treatment.”
In the caption she gave more detail, explaining she had two scraped knees, a staved thumb, a severely swollen lip and two chipped teeth; one was so far back she couldn’t close her mouth.
Showing true grit, she completed another 1.5miles after the incident to finish her route.
Diane and her son Ross kept their familial connection a secret in series twoCredit: BBC
She wrote: “My tooth was masterfully maneuvered back into place and treatment completed with an orthodontic wire.”
Her followers were quick to comment, wishing her well and praising her strength for returning to exercise so soon after the accident.
One wrote: “Yikes! Not sure I would have carried on after that…”
Diane replied: “I’m a tad bloody minded – matching my face this morning!”
Another said: “Ouch!!!! But obviously finish the run! hope you’re ok.”
The reality star responded: “I’ll live, thank u. Tooth mightn’t though!”
In another exchange, a fan posted: “Poor you! Sounds painful… hope it doesn’t impede the rose enjoyment.”
Diane said: “Rarely impeded – even if I have to use a straw to accommodate a swollen mouth!!!”
The previous day, the retired teacher shared a picture with her son Ross, with whom she appeared in The Traitors with.
She wrote: “Lovely meeting up with Ross and Rima and what a great holiday destination – Lisbon!”
“Plenty of sunshine, running, exploring, shopping, Padel AND the discovery of natural wines! We arrived just in time for the start of Festas de Lisboa – so lots of craic!”
The series two pair were responsible for one of the series’ biggest twists and were both a big hit with viewers.
Their co-stars had no idea they were related until Ross delivered the news after being eliminated at the round table in episode 10.
His parting words were: “I am a Faithful… oh wait, no, I’m a Traitor. But I was a Faithful for most of it. And I do have one more secret… Diane is my mum.”
PROVIDENCE, R.I. — A federal judge has blocked the Trump administration’s sweeping demands for confidential transgender patient information from Rhode Island’s largest hospital that provides gender-affirming care to minors.
U.S. District Judge Mary McElroy’s Wednesday ruling is the latest setback for the U.S. Department of Justice, where at least seven other federal courts have agreed to quash or limit the expansive civil subpoenas sent to more than 20 doctors and hospitals last summer.
McElroy’s decision also echoed similar concerns raised by judges surrounding the expansive scope of the subpoenas, describing the Justice Department as having “immense prosecutorial authority and discretion” but no longer trustworthy it will enforce its power fairly and honestly.
“DOJ has proven unworthy of this trust at every point in this case,” McElroy wrote.
A Justice Department spokesperson said Thursday that it would appeal and continue with its investigations.
“The Rhode Island court’s attack on the professionalism and integrity of DOJ attorneys is outrageous and unjustified,” the department said.
According to the subpoenas, the Justice Department had demanded Rhode Island Hospital hand over the birth dates, Social Security numbers and addresses of every patient who received transgender care over the past five years. It also included instructions to provide all documents detailing adverse side effects in minor patients who received gender-related care, assessments that formed the basis for prescribing puberty blockers or hormone therapy, as well as patient intake forms and guardian authorization.
The Justice Department has repeatedly argued that the information sought in the subpoenas is needed to investigate possible fraud or unlawful off-label promotion of drugs. Most recently during a hearing in Rhode Island, the DOJ said that the investigation was taking place in the Northern District of Texas, where the court’s chief judge ordered Rhode Island Hospital to comply with the subpoena before McElroy’s decision voided the subpoena.
Assistant U.S. Atty. Brantley Mayers told McElroy during the hearing that the Justice Department is investigating potential “misbranding” of drugs approved by the U.S. Food and Drug Administration, such as puberty blockers for young people. While off-label prescribing is legal, Mayers said that the DOJ is concerned that pharmaceutical companies are providing “financial incentives” to Rhode Island doctors to prescribe the drugs.
The subpoenas were crucial in getting the names of children and their families so the Justice Department could interview them.
McElroy rejected that argument.
“The administration has publicly characterized gender-affirming care for minors as abuse, directed the DOJ to bring its practice to an end, and celebrated when hospitals curtailed such programs as a result of this subpoena campaign,” McElroy wrote.
The Rhode Island decision is the latest development in the fight over transgender youth health records. Earlier this week, 11 families filed a class-action lawsuit seeking to block the Justice Department from obtaining the documents. The lawsuit, filed in Maryland’s federal court, is backed by families with transgender children who have received care from hospitals across the U.S.
And separately, a New York hospital announced that it received a grand jury subpoena from federal prosecutors in Texas seeking information about children who received gender-affirming care and the medical providers who administered it.
NYU Langone is the first hospital system to publicly acknowledge receiving a subpoena for such records as part of a federal criminal investigation. But the institution said in its statement Tuesday it was one of several that received a subpoena out of the Northern District of Texas on May 7. It said it was deciding on how to respond.
“The government cannot use its subpoena power to intimidate families out of seeking lawful medical care. To trans and gender-diverse children and their families, we want you to know that you are valued, you are not alone,” Kevin Love Hubbard, an attorney with the Lawyers’ Committee of Rhode Island, who represented the plaintiffs in the case, said in a statement.
Gender-affirming care includes a range of medical and mental health services to support a person’s gender identity, including when it’s different from the sex they were assigned at birth. It may include counseling, medications that block puberty, hormone therapy to produce physical changes or surgeries to transform chests and genitals, although those are rare for minors.
Most major medical groups say access to the treatment is important for those with gender dysphoria and see gender as existing along a spectrum.
At least 27 states have adopted laws restricting or banning the care for minors, while several others have adopted laws or policies protecting access to transgender healthcare.
“In Q1, our performance was consistent with the expectations we outlined on our last call.” (President, CEO, Secretary & Director Evert Schimmelpennink) “We delivered approximately 25,000 paid and filled prescriptions… and generated $1.9 million in net revenue, including $1.7 million in
Seeking Alpha’s Disclaimer:This article was automatically generated by an AI tool based on content available on the Seeking Alpha website, and has not been curated or reviewed by humans. Due to inherent limitations in using AI-based tools, the accuracy, completeness, or timeliness of such articles cannot be guaranteed. This article is intended for informational purposes only. Seeking Alpha does not take account of your objectives or your financial situation and does not offer any personalized investment advice. Seeking Alpha is not a licensed securities dealer, broker or US investment adviser or investment bank.
A humanoid robot jointly developed by KB Financial Group and GENON is demonstrated at the AI EXPO Korea 2026 in Seoul on Friday. Photo by KB Financial Group
SEOUL, May 10 (UPI) — South Korea’s KB Financial Group unveiled a humanoid robot for senior care during AI EXPO Korea 2026 held in southern Seoul.
During the three-day event last week, KB Financial showcased the humanoid robot, named “GenP,” which was jointly developed with domestic AI company GENON.
KB Financial noted that GenP was specifically designed for senior care, as it is equipped with upgraded finger-module capabilities to perform precise movements suited for assisting elderly users.
During the exhibition, the humanoid robot carried out five demonstrations, including greeting visitors and delivering daily information, such as rehabilitation schedules.
The Seoul-based financial conglomerate said that the presentation demonstrated its transition from text-based agentic AI to physical AI geared toward engaging directly with the everyday lives of senior customers.
Next month, KB Financial’s affiliate plans to introduce an AI-powered care robot, dubbed “KeBi,” at a South Korean facility for senior citizens.
South Korea is widely regarded as having one of the world’s fastest-aging societies, as the proportion of people age 65 or older topped 20% of the population. As of the end of last year, it was 21.21%, according to the Ministry of the Interior and Safety.
“Starting with this demonstration, we plan to gradually verify the feasibility of applying physical AI to care settings. Based on those results, we will further expand our service scope and business operations,” KB Financial said in a statement.
“Going forward, we will concentrate our capabilities on realizing the future of senior care solutions, which combine advanced technology and compassionate care,” it said.
The share price of KB Financial rose 0.31% on the Seoul bourse Friday.