


Goma, Democratic Republic of the Congo – It’s dawn at the mpox treatment site at Nyiragongo General Referral Hospital, north of the city of Goma, and Congolese medics are already hard at work, calmly and efficiently screening, isolating and caring for patients infected with the disease.
Two days prior, the World Health Organization (WHO) issued its highest alert level for mpox after the African Africa Centres for Disease Control and Prevention (Africa CDC) declared the viral disease previously known as monkeypox a continental emergency.
But for doctors in DRC – who have been tackling the latest mpox outbreak since 2022 amid medicine shortages, an ongoing rebellion in the east, and after years toiling on the front lines of Ebola epidemics – the challenges have become routine.
In between the stream of patients visiting the Nyiragongo Hospital for all number of ailments, teams of hygienists and other health providers tend to mpox patients in a separate white tented area where those suffering from the highly infectious disease can be isolated to avoid any risk of contamination.
Among them, shopkeeper Madam Nyota Joyeuse is resting in a small three-bed tent. The 35-year-old mother of two fell ill about a week prior.
She had a headache, fever, muscle aches and a slight flu, so assumed it was malaria, which is common in North Kivu. But when her symptoms weren’t easing days later, she finally came to the clinic.
“I felt as if the whole universe had fallen on my head when I was told I had monkeypox,” she tells Al Jazeera, worried that her health had deteriorated and her business would come to a halt.
But the treatment she’s receiving is helping her. “Fortunately, that’s promising. May the Almighty bless those who take care of us,” she says from her hospital bed.


‘Monkeypox’ to mpox
Originally named “monkeypox” when it was first identified in monkeys in 1958, the name of the disease was updated to “mpox” in 2022 to reduce stigma.
Endemic to parts of Central and West Africa, mpox is related to the virus that caused the now-eradicated smallpox, and can be fatal in severe cases.
Although outbreaks are common in DRC, health experts say the recent rise is due to a new strain, clade 1, that is spreading faster and wider than ever before.
This week, the WHO said cases have been detected in 13 African countries, as well Sweden, Pakistan and the Philippines.
The Africa CDC said cases are up 160 percent in 2024 compared with the same period last year.
In DRC the disease has been detected in all 26 provinces. As of last week, the country recorded more than 15,000 cases of mpox, resulting in 548 deaths this year.
Badiambila Mulumba, the medical director of Nyiragongo Hospital, tells Al Jazeera his facility began treating mpox this June, and has since registered 278 cases referred to them – “both positive and negative cases”, he says.
As of August 10, there were 78 positive cases at his facility, but no deaths.
“We continue to control cases. There are mild and serious cases, but no deaths,” he tells Al Jazeera.

Ebola, COVID, mpox
Rachel Maguru is an attending physician at the North Kivu Provincial Hospital, another government facility, in downtown Goma, where she treats mpox patients.
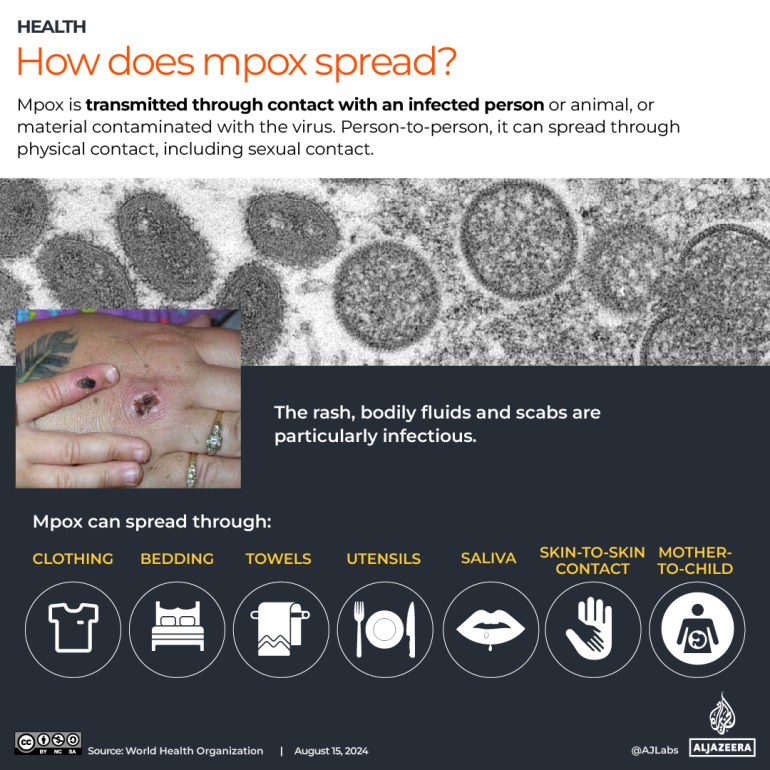
She tells Al Jazeera many people arrive for treatment only after the disease manifests on their skin. Mpox causes a distinctive rash that eventually forms pustules.
“What’s real is that many patients don’t discover the disease early on. They become aware of it once their skin manifests an unusual form of gall,” Maguru says, concerned.
The hospital where she works had treated 10 positive cases up until August 10, all of which were declared cured. She takes this as a positive sign that all mpox patients in her care will recover and circumstances around the disease will improve.
“We’re not under pressure from this pandemic. We’ve [previously] had to deal with others like Ebola and coronavirus. With this experience behind us, we’re also facing this mpox,” she says.
This part of eastern DRC was home to an Ebola treatment centre during the 10th outbreak of that epidemic, which claimed more than 2,000 lives between 2018 and 2020. Health workers here have experienced some of the most challenging work environments, so many feel they can tackle mpox too.
Unlike during other epidemics, however, authorities in DRC have not yet imposed restrictions or lockdown orders. Activities are proceeding normally in every sector in Goma. But some people say this makes them worry about the spread of mpox.
“I’ve heard that the WHO has declared mpox an international health emergency, and I’m already worried, especially as our health system has been weakened by Ebola and COVID-19. We have to do everything we can to limit the spread of the disease,” Herve Murhula, 26, a street seller in Goma, tells Al Jazeera.
On the other hand, Merveille Uwezo, a final year high school student, says she is praying that the advent of mpox will not hinder the school year, which starts in September.
“I’ve heard on social networks that there’s a contagious disease called monkeypox, and it scares me. During COVID-19, we stopped classes, and now my fear is that maybe mpox will affect our school programme,” she says sombrely.

Conflict in the east
For many health workers and NGOs in North Kivu, there is a bigger challenge that they worry could hinder their ability to respond to the mpox outbreak: conflict.
In recent years, M23 rebels have been facing off against the Congolese army and fighters from local self-defence militias as the rebels try to gain territory from the government. This has led to deaths and displacement, and has also cut off access to communities in areas where there is fighting.
Since 2022, North Kivu has been facing a cholera epidemic in camps for internally displaced people around Goma, due to precarious hygiene conditions there. A measles epidemic has also been reported in other parts of the country. And now mpox is escalating.
This situation is of concern to medical NGO Doctors Without Borders, known by its French initials MSF, which supports the Congolese government in the fight against mpox in the provinces of North Kivu, South Kivu and Equateur.
The NGO says it’s treated more than 1,100 cases of mpox in the three provinces, despite the complex humanitarian and conflict situation in eastern DRC.
Natalia Torrent, head of the MSF team in Mweso near Goma, fears that the current conflict could have a negative impact on efforts to combat the disease and the aid organisation’s ability to respond as well as it hopes to.
“Will we really be able to manage all these epidemics at the same time, especially as the situation is worsened by the humanitarian crisis in the region, with the proliferation of camps for war-displaced people around Goma,” Torrent wonders.


Treating the symptoms
At the mpox treatment site in Nyiragongo, mother of six Amina Upendo, 40, waits for her daughter to recover.
Her 10-year-old, Yvette, lay in her hospital bed last week struggling with the disease. Upendo says she had difficulty detecting that it was mpox at first, also believing it to be malaria because of some similar symptoms.
“We noticed that she had an unusually high fever and a headache,” she explains. “Two days later, she developed a scab on her skin. That’s when, thanks to advice from neighbours, we were sent here to the treatment site,” she adds, appreciative of the care her daughter is now receiving.
But even when people seek treatment, the drugs are not always available.
Nzayinambaho Theophile, a healthcare provider at Nyiragongo Hospital, admits that at times, stockouts of medicines at the site slightly delays patient treatment.
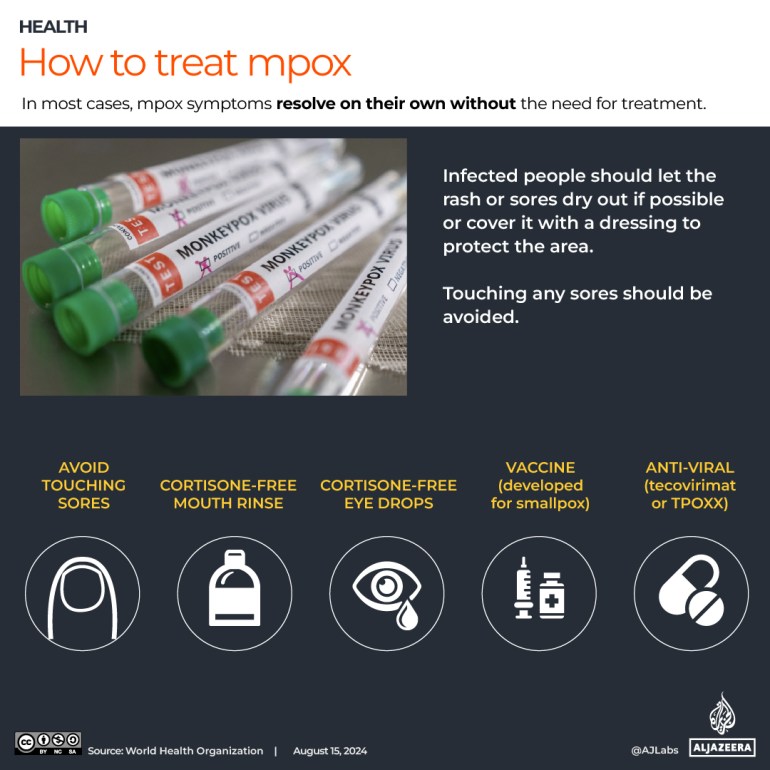
Additionally, no special treatment is even available to treat cases of mpox in DRC. Although some antiviral drugs are being tested internationally, they are not yet available here.
Congolese health authorities have instead had to adopt a protocol of alleviating a patient’s symptoms.
“We treat patients based on the symptoms they present. For example, if they have headaches, we treat these concerns with paracetamols. If they have skin problems, we call in dermatologists, and we’ve been able to measure a certain number of [positive] results,” says Maguru, the physician at North Kivu Provincial Hospital.
But with stockouts, even basic remedies sometimes fall short.
For prevention, although there is a vaccine in existence (originally developed for smallpox) that can help reduce the risk of contracting mpox, this is not available to the most at-risk in DRC. It’s something experts and some African leaders blame on vaccine inequality and the stockpiling by Western countries that was also witnessed during the COVID pandemic.
The vulnerable ‘pay the price’
So far, the lethality rate linked to mpox is more than 3.5 percent, and this is creating concern among civil society members in the health sector in North Kivu.
Emmanuel Bitangalo, a health activist, is concerned about the way the disease is spreading, and fears the possible “serious consequences” it could have on the life of the nation.
He proposes that authorities put in place an emergency response plan to counter mpox, and increase public awareness of the disease.
The Congolese government, however, says the country is doing what it can.
In a press briefing last week, Health Minister Roger Kamba said the government has “activated all necessary mechanisms to identify and treat cases free of charge”.
He added that DRC needs nearly three million doses of vaccinations to limit the spread of the disease, saying the country has already “ordered” them. But he also expressed concern that vaccines against the epidemic are “very expensive”, and called on partners to lend a hand to the country.
Meanwhile, in North Kivu, Congolese authorities have not yet announced concrete measures to specifically combat mpox in the midst of the ongoing conflict and displacement crisis.
Rodriguez Kisando is a doctor in public health, specialising in the field of environmental health risk assessment methods and tools.
He believes that mpox – and previous epidemics – call into question the state of the health system in DRC, which as in the rest of Africa, faces various challenges.
“The authorities need to define and put into practice a concrete policy linked to human, animal and environmental health,” he advises.
“The corollary of war is that displaced people risk paying the price of this disease as they live in precariousness,” he adds.